
CLN - Focus on Laboratory Stewardship
Supported By

In the evolving landscape of precision oncology, the gap between clinical guidelines and real-world practice presents a persistent challenge. For patients with non-small cell lung cancer (NSCLC), comprehensive molecular profiling is widely recognized as the standard of care, which enables clinicians to identify actionable mutations and guide targeted therapies (1,2). Yet in day-to-day practice, many oncologists still rely on single-gene assessments or fluorescence in situ hybridization (FISH) testing — often in an effort to reduce costs or accelerate results.
At the University of Washington (UW) Medical Center in Seattle, this well-intentioned approach created a cascade of unintended consequences.
In this article, we describe how the genetics division leadership and program operations team within the UW department of lab medicine and pathology addressed these issues in 2024 and 2025, enabling our institute to consistently provide comprehensive molecular profiling to patients with lung cancer.
At first, oncologists’ preference for single-gene and FISH testing appeared practical. However, these tests often failed to provide the comprehensive insights needed to make treatment decisions and led to additional rounds of testing and longer overall timelines.
The impact was felt most acutely in the cytogenetics laboratory, where a surge in ALK and ROS1 FISH orders strained capacity. Turnaround times for critical STAT testing increased, and what should have been a streamlined process became an increasingly reactive one.
Because these limited tests reported on only a handful of genes, molecular directors and ordering providers were frequently drawn into case-by-case discussions to determine which results should be prioritized. Preliminary report emails, once an exception, became routine. Meanwhile, thoracic oncology cases required repeated workflow exceptions and disrupted standardization across the system.
Although the challenges were multi-factorial, the UW genetics division was uniquely positioned to respond to interconnected inefficiencies in a coordinated way with centralized leadership across molecular diagnostics, cytogenetics, and supporting teams. This unified oversight became the foundation for meaningful change, ensuring that improvements in one area would translate across the entire testing ecosystem.
A critical early step was engaging clinical leadership. Change in laboratory processes cannot succeed without clinician buy-in, particularly when it affects ordering practices.
The thoracic oncology service line director, Keith Eaton, MD, played a pivotal role in this effort. As a trusted clinical leader, he bridged the gap between laboratory operations and provider concerns. By clearly articulating the benefits of comprehensive molecular profiling — not only for workflow efficiency but also for patient outcomes — he helped bring physicians into alignment. His leadership ensured that the transition was both decisive and cohesive.
Despite these efforts, one fundamental question remained: where, exactly, were delays occurring?
Traditional turnaround-time metrics provided only a partial view, often failing to capture the full journey from test order to final report. Without this visibility, it was difficult to prioritize interventions or measure progress.
The solution was the development of a somatic metric dashboard — a tool that would become central to the division’s transformation (see Figure 1). Launched in the second quarter of 2024, the dashboard established baseline performance metrics and tracked turnaround times across the entire testing process. It also enabled comparison against clinical benchmarks, including recommended timelines for genomic testing and treatment initiation.
Figure 1. The somatic metric dashboard
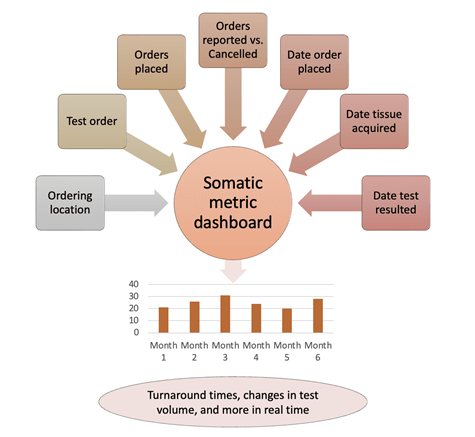
For the first time, teams across multiple laboratories were working from the same data. This fostered accountability, aligned priorities, and created a common language for discussing performance.
The dashboard’s real impact came from how the data was used. In the third quarter of 2024, the division introduced a Turnaround Time Outlier Report, which was built directly from the dashboard. Each month, cases that exceeded expected timelines were reviewed.
What followed was a disciplined, collaborative process. Pre-analytical and analytical teams examined each outlier to identify root causes — whether delays stemmed from specimen acquisition, processing workflows, sequencing schedules, or reporting practices.
These findings were then synthesized and presented to senior leadership to create a direct link between frontline observations and strategic decision-making. Importantly, the focus remained on the most impactful tests and the most frequent sources of delay to ensure that efforts were targeted and effective.
One of the most striking outcomes of the outlier review process was the realization that meaningful improvements did not always require major investments.
Several operational adjustments delivered immediate results. Increasing sequencing runs from once to twice per week expanded capacity and reduced backlog. Adjusting sign-out schedules to ensure two directors were available to review results minimized reporting delays. Together, these changes reduced turnaround time by 12 calendar days — a substantial improvement achieved with relatively modest effort.
Additional refinements, including targeted staffing increases and improvements in tissue acquisition processes, further strengthened performance.
The outlier reports also brought attention to less obvious bottlenecks. Holiday weeks, for example, consistently showed increased turnaround times. The issue was not the holiday itself, but the reduction in sequencing runs during those weeks.
By maintaining two runs per week, regardless of holidays, the laboratory eliminated an average of six delays per month — demonstrating how data can drive effective solutions for problems that may have otherwise been overlooked.
Specimen transport presented another opportunity. Reliance on standard shipping introduced variability and delays, particularly for samples arriving from external partners. Implementing a dedicated courier system streamlined this process and improved overall reliability.
Beyond the operational gains, this initiative reshaped how the division approached problem-solving. The combination of unified leadership, transparent data, and structured review created a culture of continuous improvement.
Teams were no longer reacting to issues in isolation. Instead, they were working collaboratively, guided by shared metrics and a clear understanding of system-wide performance.
The presence of a single division head overseeing multiple laboratories was instrumental in sustaining this culture. It ensured that improvements were coordinated, priorities remained aligned, and progress in one area reinforced the progress in others.
At the same time, efforts were under way to address barriers outside the institution. Insurance coverage and prior authorization requirements often influence testing decisions, sometimes steering providers toward less comprehensive options.
Engagement with patient advocacy groups and participation in legislative discussions helped shape a more supportive environment for molecular testing.
The transformation of molecular testing workflows at our institution offers a compelling example of what can be achieved when leadership, data, and collaboration come together (see Figure 2).
Figure 2. Key elements for transforming molecular testing workflows
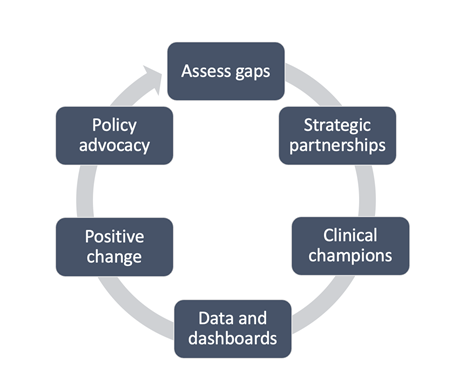
The somatic dashboard provided the visibility needed to understand performance. The outlier review process created focus and accountability. And unified oversight enabled the rapid, system-wide implementation of solutions.
Most importantly, these efforts translated into better outcomes for patients. They delivered faster, more comprehensive results and supported timely, informed treatment decisions.
Alyssa Johnson, MBA, is the program operations manager of genetics revenue at the University of Washington Medical Center in Seattle. +Email: [email protected] Emily A. Malouf, MGC, is a lab stewardship genetic counselor in the department of laboratory medicine and pathology at the University of Washington in Seattle. +Email: [email protected]