
CLN - Industry Insights
Sponsored By
![]()

Blood analysis is a cornerstone of diagnostic medicine, with serum and plasma serving as the primary matrices for a wide array of laboratory tests. Accurate clinical interpretation relies not only on the analytes being tested, but also on the appropriate specimen type and tube selection. BD Vacutainer® Blood Collection Tubes, specifically serum separator tubes (SST™), lithium heparin plasma separator tubes (PST™), and rapid clot serum tubes (RST™) are three tube types commonly used in routine clinical chemistry testing. Each tube type has unique characteristics that impact sample preparation, processing time, and test compatibility. Understanding the specific properties and appropriate use of these tubes can improve laboratory efficiency and patient care. This article provides a comprehensive comparison of these tubes, highlighting their differences, advantages, and limitations to support informed selection in clinical laboratory settings.
Serum is the clear, yellowish fluid portion of blood that remains after blood has clotted and the clot (including blood cells and clotting proteins like fibrinogen) has either been removed or separated via gel/barrier. It contains water, electrolytes, hormones, antibodies, antigens, and other proteins—except for the clotting factors. Serum is often used in routine clinical chemistry and serology testing.
Plasma, in contrast, is collected by centrifuging a blood tube containing an anticoagulant (e.g. heparin, ethylenediaminetetraacetic acid [EDTA], and citrate) thus preserving clotting factors within the liquid component. Citrated plasma is typically used in coagulation studies, such as prothrombin time (PT) and activated partial thromboplastin time (aPTT), and in certain biochemical tests where clotting proteins may be necessary or where sample stability is a concern.
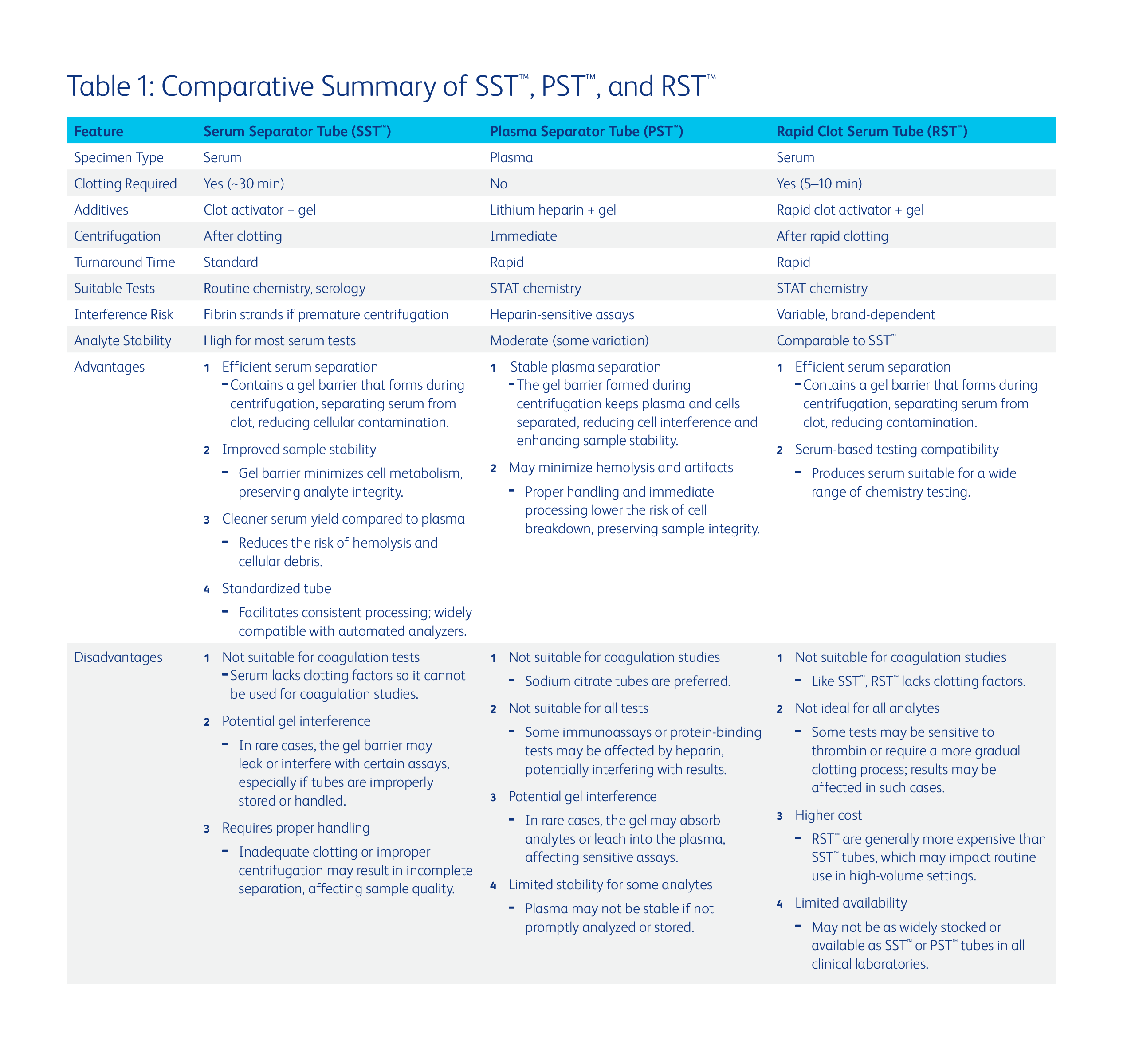
Modern clinical chemistry laboratories rely on specialized collection tubes to streamline the processing of serum and plasma samples. Three widely used tubes include: SST™, PST™, and RST™ (Table 1). SST™ are designed to collect serum after coagulation and centrifugation. They typically contain a clot activator and a gel barrier that separates serum from the clot during centrifugation. After collection, the sample must sit undisturbed for approximately 30 minutes to allow full clot formation prior to centrifugation. PST™ contain lithium heparin, an anticoagulant that prevents blood clotting, along with a gel separator. These tubes allow immediate centrifugation and separation of plasma, significantly reducing turnaround time. RST™ are designed to accelerate the clotting process, often using thrombin-based clot activators. These tubes typically allow clotting within 5 to 10 minutes, facilitating faster serum separation for urgent testing.
The distinctions between serum/plasma and the various tubes available must be carefully considered when deciding to implement a specific specimen or tube type in the laboratory. In general, tube selection should be guided by the test, urgency, and analytical method. Additionally, the impact on preanalytical variables should be considered when selecting a tube type. Serum is the most widely used specimen type for routine chemistry testing due to broad assay compatibility (1). However, there are several documented examples where one specimen or tube type confers a particular benefit over another.
Serum or SST™ specimens have been shown to offer better stability for some analytes when compared to plasma or PST™. For example, studies have demonstrated that the stability of glucose is greater in serum than in plasma samples stored at room temperature due to a lower degree of metabolism occurring in serum that is devoid of cells (1). Additional evidence highlights the risk of leucocytosis-induced plasma hyperkalemia upon pneumatic tube transport which can be mitigated through use of serum tubes (2).
The strongest arguments for the use of PST™ are made in the context of turnaround time and specimen yield. Plasma samples can be centrifuged immediately after collection. However, if a serum specimen is centrifuged before clot formation is complete (~30 min), residual fibrin or fibrinogen may interfere with instrument operation/testing and could lead to inaccurate results (3,4). Short turnaround time (TAT) is necessary to ensure appropriate therapeutic treatment in urgent patient care settings, specifically in the Emergency Department, operating rooms, and intensive care units. The use of PST™ can facilitate rapid result reporting in these time-sensitive scenarios. Plasma may also be the ideal choice when specimen volume is of concern. Centrifugation of anticoagulated specimens yields approximately 15-20% more volume compared to serum (1). This enables the use of low volume tubes which have been shown to reduce iatrogenic anemia in patient populations with reduced blood volumes (e.g. low birthweight infants) (1).
Recent publications have highlighted the efficacy of RST™, specifically in reducing preanalytical errors compared to traditional collection methods, while maintaining a short TAT (5–7) . A recent study conducted at Yale New Haven Hospital assessed the impact of tube type, fill volume, and collection methods on hemolysis and high-sensitivity cardiac troponin T (hs-cTnT) testing (5). The findings indicated that RST™ significantly reduced hemolysis compared to PST™. Proper tube filling further decreased hemolysis, underscoring the importance of correct collection techniques. Additionally, RST™ demonstrated a lower false positive rate for hs-cTnT levels <50 ng/L, suggesting improved assay accuracy in hemolyzed samples (5). A study comparing RST™ with traditional SST™ found that RST™provided shorter clotting times and were also less prone to hemolysis than SST™tubes (8). RST™ produced similar baseline results as SST™, consistent with other reports (9,10), making them a viable alternative for reducing processing time while maintaining sample quality.
To ensure optimal sample quality and test accuracy, consider the following best practices:
The selection of the appropriate blood collection tube is crucial in clinical chemistry laboratories to ensure timely, accurate, and reliable test results. By understanding the characteristics, applications, and limitations of SST™, PST™, and RST™, laboratory professionals can make informed decisions that optimize patient care and laboratory efficiency. Optimal use depends on balancing speed, assay compatibility, and analyte stability. Adhering to best practices in tube selection and handling can significantly reduce preanalytical errors, improve the overall quality of laboratory diagnostics, and enhance patient outcomes.
Industry Insights articles are created and paid for by advertisers. The views expressed in these articles do not necessarily represent ADLM's views, and their inclusion in CLN is not an endorsement by CLN or ADLM.
![]()