
Academy of Diagnostics & Laboratory Medicine - Guidance Document
Guidance Documents are brought to you by the

Tiffany A. Thomas
Department of Pathology and Cell Biology
Columbia University
New York, NY
Gabrielle N. Winston-McPherson
University of Wisconsin
Madison, WI
Ina Amarillo
Department of Pathology and Laboratory Medicine
Hershey, PAPenn State Health
Alisha D. Berry
Department of Laboratory Medicine & Pathology
University of Washington
Seattle, WA
Caroline J. Davidge-Pitts
Division of Endocrinology, Diabetes and Nutrition
Mayo Clinic
Rochester, MN
Sridevi Devaraj
Department of Pathology
Baylor College of Medicine and Texas Children's Hospital
Houston, TX
Zil Goldstein
Callen-Lorde Community Health Center
Brooklyn, NY
Brad S. Karon
Department of Laboratory Medicine and Pathology
Mayo Clinic
Rochester, MN
Brooke M. Katzman
Department of Laboratory Medicine and Pathology
Mayo Clinic
Rochester, MN
Department of Laboratory Medicine and Pathology
University of Minnesota
Minneapolis, MN
Hung S. Luu
Department of Pathology
Children’s Health
Dallas, TX
James H. Nichols
Vanderbilt University Medical Center
Nashville, TN
Tracy L. Stockley
Laboratory Medicine Program
University Health Network and University of Toronto
Toronto, Ontario, Canada
Michelle R. Stoffel
Department of Laboratory Medicine and Pathology
University of Minnesota
Minneapolis, MN
Dina N. Greene
Department of Laboratory Medicine & Pathology
University of Washington
Seattle, WA
Matthew D. Krasowski
Department of Pathology
University of Iowa Health Care
Iowa City, IA
Drs. Thomas and Winston-McPherson are co-first authors.
Drs. Greene and Krasowski are co-corresponding authors and co-chaired this project.
This document was approved by the Academy Content Development Committee and Academy Council in February 2026 and the ADLM Board of Directors in March 2026.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted reuse, distribution, and reproduction in any medium, provided the original work is properly cited.
The first international clinical standards of care for the gender-diverse population were formulated in the late 1970s. In the last 15 years, multiple subspecialty societies within the United States have developed clinical care guidelines for those with gender dysphoria, including gender-affirming hormone therapy (GAHT) and surgical treatments. To date, there are no pathology- and laboratory medicine–specific recommendations in the United States for the gender-diverse population.
This document outlines pathology- and laboratory medicine–specific recommendations for providing optimal care to the gender-diverse population, with a predominant focus on the adult population. The scope of this document focuses on the following 5 topics: (a) reference intervals and interpretation of laboratory tests impacted by use of GAHT (testosterone for transgender men; estradiol with or without antiandrogens for transgender women), focusing on those stably on GAHT for 6 months or longer; (b) transfusion medicine considerations for the gender-diverse patient population, (c) consideration of gender diversity in autopsy and death investigation, (d) interpretation of histology from tissues that are impacted by GAHT and surgical procedures; and (e) pathology and laboratory medicine informatics challenges and opportunities.
Summary:
A relatively small group of laboratory tests is significantly impacted by GAHT. The histology of some tissues shows changes attributable to GAHT or to nonhormonal medical procedures. Autopsy and transfusion medicine practices for the gender-diverse population currently lack standardization, although this is evolving. The landscape of pathology informatics related to gender diversity is complicated by varying electronic health record and laboratory informatics systems functionality. Abbott Diagnostics10.13039/100014386Roche Diagnostics10.13039/100016545
The first systematic series of medical and scientific manuscripts related to gender variance was published in the 1950s and 1960s (1). The first published clinical standards of care for what is now termed gender dysphoria were published in 1979 by the Harry Benjamin International Gender Dysphoria Association, Inc., which later became the World Professional Association for Transgender Health (WPATH) (2). The WPATH Standards of Care are now in its eighth version (3). Over the last 15 years, numerous medical societies within the United States have published guidelines or recommendations related to clinical care of the gender-diverse patient population, including endocrinology (4, 5), pediatrics (6), plastic surgery (7), and urology (8).
In Australia, best practice guidelines for pathology testing for transgender and intersex (differences of sex development) individuals have also been published (9).
Within the United States, there have been efforts to provide guidance on handling of surgical specimens collected from transgender and intersex patients, as well as for specimens arriving with either missing or unknown gender or sex markers (10). A working group of the Association for Molecular Pathology recently provided recommendations and considerations for sex- and gender-inclusive collection of specimens for cytogenetics and molecular genomics testing (11, 12). However, to date, there are no published specific recommendations in the United States that broadly cover laboratory medicine, anatomic pathology, and pathology informatics.
To address this need, an expert panel was convened to review the literature as it relates to clinical laboratory and regulatory frameworks. Members included clinical and anatomic pathologists; PhD laboratory medicine experts with training and board certification in areas such as clinical chemistry, laboratory genomics, and molecular genetics; and primary care and endocrinology providers involved in direct clinical care of transgender patients. Panel members were selected to represent geographically diverse institutional environments, including academic medical centers, reference laboratories, and private institutions, to ensure that multiple perspectives were represented. The expert panel met periodically via teleconference as a large group. Subgroups within the broader panel focused on specific areas: anatomic pathology, impact of hormone therapy on laboratory test results and reference intervals, transfusion medicine, and informatics. The objective of this publication is to outline the medical needs of adult transgender people as they specifically relate to laboratory medicine and pathology. Basic definitions relevant to this document are listed in Table 1. Throughout the document, we refer to people using gender-affirming hormones as transgender and are inclusive of nonbinary people within this umbrella term, although some nonbinary people may not identify as transgender.
Table 1. Definitions.
| Term | Definition |
| Administrative sex | Sex designation used for administrative purposes, such as medical documentation and health insurance billing |
| Chosen or correct name | Refers to the name a person uses that aligns with their gender identity |
| Gender | Social and cultural constructed identities, roles, behaviors, and expectations associated with individuals, which may or may not align with the sex they were assigned at birth |
| Gender diverse | Umbrella term for individuals whose gender identity or expression differs from traditional expectations based on the sex assigned to them at birth. This includes, but is not limited to, people who identify as transgender, nonbinary, genderqueer, genderfluid, or other identities beyond the male/female binary. The terms transgender and gender diverse are also commonly used as broad and inclusive descriptors. |
| Gender dysphoria | Psychological distress resulting from gender identity being different from SAAB. This distress could relate to one’s body, social roles, and/or how they are perceived by others. |
| Gender identity | A person’s deeply held internal sense of their own gender, which may be male, female, a blend of both, or another identity altogether. It may or may not align with the sex assigned to them at birth. |
| GAHT | Medical therapy used to affirm gender identity. The most common medications are testosterone for transgender men and estradiol, often with antiandrogens (e.g., spironolactone, CPA, finasteride), for transgender women. |
| Gender-affirming surgeries | Medical procedures that help align a person’s physical body with their gender identity |
| Intersex | Individuals born with physical sex characteristics, such as chromosomes, gonads, hormones, or genitalia, that do not fit typical binary notions of male or female bodies. These natural variations are sometimes medically referred to as differences of sex development. |
| Legal sex | Sex designation recorded on an individual’s official documents, such as motor vehicle licenses and passports. Legal sex is the main sex designation used for medical records and procedures/documentation that use logic based on a male/female binary. The process for changing legal sex varies depending on local, national, and institutional laws and policies. |
| Nonbinary | A person whose gender identity exists outside the conventional categories of man and woman and may include a mix of genders or no gender |
| Organ inventory | A table or checklist within the EHR that documents the presence or absence of specific organs and dates of surgical procedures. It supports accurate, individualized clinical care by reflecting a patient’s current anatomy regardless of legal sex or gender identity. |
| Pronouns | The words used to refer to someone in place of their name, such as he/him, she/her, or they/them |
| Sex | The classification of individuals as male, female, or intersex based on biological characteristics, including chromosomes, hormone levels, and reproductive or sexual anatomy. While often assigned at birth, biological sex exists along a spectrum and may not always align with a person’s gender identity. |
| SAAB | Classification of an individual as male, female, or intersex based on physical characteristics observed at birth, typically through external genital examination. In some cases, additional diagnostic studies such as chromosomal or hormonal testing may be used. SAAB is used as the sex designation on newborn birth certificates. |
| SOGI fields | Fields in the EHR where patients can voluntarily identify SAAB, gender identity, sexual orientation, pronouns, and other related information |
| Transgender | A person whose gender identity differs from their SAAB |
| Transitioning | The personal, social, and/or medical steps a transgender person may take to live in alignment with their gender identity. This can include changes in name, pronouns, appearance, clothing, legal documents, hormone therapy, and/or surgeries. Each person’s transition journey is unique and may involve some, all, or none of these steps. |
| Transgender man/trans man | Someone whose SAAB is female but identifies as male |
| Transgender woman/trans woman | Someone whose SAAB is male but identifies as female |
This guidance document intends to (a) review evidence for how gender-affirming hormone therapy (GAHT) impacts laboratory tests and the significance of these changes and propose reference intervals and interpretation for selected clinical laboratory tests for those stably on GAHT for 6 months or longer, (b) discuss transfusion medicine considerations for the gender-diverse patient population, (c) outline best practices related to documentation of gender diversity in autopsy and death investigation, (d) summarize available knowledge on the hormonal and non-hormonal impacts of gender-affirming treatments on cytology and tissue histology, and (e) outline informatics challenges and opportunities for the gender-diverse population including utilization of sexual orientation/gender identity (SOGI) fields within electronic health record (EHR) and laboratory information system (LIS) software.
This guidance focuses on the adult gender-diverse population. For the topics covered in this guidance document, the available literature is evolving and often incomplete, inviting opportunities for future studies. Prospective studies and systematic reviews are relatively rare, although some have been published in recent years (13–20). This guidance document also highlights gaps where additional studies are needed.
Standard of care for transgender women and men who choose to medically transition includes feminizing GAHT (estradiol with or without antiandrogen medication like spironolactone, finasteride, or cyproterone acetate [CPA]) and masculinizing GAHT (testosterone), respectively (3, 5). This section summarizes available evidence on how GAHT impacts common laboratory assays and applies to those stably on GAHT, defined here as 6 months or longer. In general, there are limited published data on the impact of GAHT on common laboratory tests at timeframes less than 6 months. This is an area for future investigation. Table 2 summarizes the key information relevant to proposed reference intervals for selected assays. Unless otherwise specified, concentrations of analytes referenced in the following discussion refer to those in serum or plasma.
Table 2. Impacts of gender-affirming masculinizing or feminizing hormone therapy on common laboratory tests, along with proposed reference intervals for interpretation.a
| Laboratory test | Impact of masculinizing therapy (testosterone) | Reference interval for transgender men | Impact of feminizing therapy (estradiol with or without antiandrogens) | Reference interval for transgender women |
| Hematology | ||||
| Hemoglobin (21, 22) | Increases | Cisgender male | Decreases | Cisgender female |
| Hematocrit (21, 22) | Increases | Cisgender male | Decreases | Cisgender female |
| RBC count (22) | Increases | Cisgender male | Decreases | Cisgender female |
| MCVa (22) | Unchanged | Not sex-specific | Unchanged | Not sex-specific |
| Platelet count (21, 22) | Unchanged | Not sex-specific | Unchanged | Not sex-specific |
| WBCb count (22) | Unchanged | Not sex-specific | Unchanged | Not sex-specific |
| Cardiac | ||||
| hs-cTn (23, 24) | Increases | Unclear | Decreases | Unclear |
| Natriuretic peptides (24) | Decreases | Not sex-specific | Increases | Not sex-specific |
| Kidney | ||||
| Creatinine (19) | Increases | Cisgender male | Unchanged | Cisgender male |
| Cystatin C (25) | Increases | Cisgender male | Decreases | Cisgender female |
| eGFR (26, 27) | Variable | Not sex-specific | Variable | Not sex-specific |
| Hypothalamus–pituitary–gonadal axis | ||||
| Estradiol (20, 28) | Decreases | Transgender specific | Increases | Transgender specific |
| Testosterone (16, 28) | Increases | Cisgender male | Decreases | Transgender specific |
| SHBG (29) | Decreases | Cisgender male | Increases | Cisgender female |
| LH (17, 18) | Variable | Unknown | Variable | Unknown |
| FSH (17, 18) | Variable | Unknown | Variable | Unknown |
| Progesterone (17, 18, 31, 32) | Decreases | Cisgender female | Variable | Transgender specific |
| Lipids | ||||
| HDL (33) | Decreases | Cisgender male | Increases | Cisgender female |
| LDL (34, 35) | Increases | Not sex-specific | Decreases | Not sex-specific |
| Triglycerides (34, 35) | Increases | Not sex-specific | Decreases | Not sex-specific |
| Total cholesterol (34, 35) | Variable | Not sex-specific | Variable | Not sex-specific |
| Liver | ||||
| ALP (33, 36, 37) | Slight increase | Cisgender male | Slight decrease | Cisgender female |
| ALT (33, 36–38) | Slight increase | Cisgender male | Slight decrease | Cisgender female |
| AST (33, 37–39) | Slight increase | Cisgender male | Slight decrease | Cisgender female |
| Tumor markers | ||||
| Prolactin (17, 18, 40) | Unclear | Cisgender female | Variable | Cisgender female |
| PSA (41) | Not applicable | Not applicable | Decreases | Transgender specific |
a Mean corpuscular volume.
b White blood cell.
Reference intervals and clinical interpretation of common coagulation assays, such as prothrombin time, international normalized ratio, activated partial thromboplastin time, and coagulation factor assays, generally do not differ between cisgender men and women, with the possible exception of protein S, and results can be interpreted independently of sex, gender, or use of GAHT (42). Although there is a complex relationship between estrogen and hemostasis, interpretation of D-dimer concentration does not differ between cisgender men and women and therefore will not differ based on the use of GAHT (43). D-dimer measurements used in algorithms for exclusion of venous thromboembolism are interpreted independently from sex (44).
Androgens stimulate erythropoiesis, resulting in different reference intervals for red blood cell (RBC) indices between postpubertal cisgender men and women. Testosterone stimulates erythropoiesis by increasing the expression of erythropoietin and iron availability (45). This leads to higher concentrations of hemoglobin, hematocrit, and RBC counts in cisgender men relative to cisgender women.
For people taking masculinizing hormone therapy, the increased testosterone concentration will lead to higher hemoglobin, hematocrit, and RBC counts that align with those seen in cisgender adult men (21, 22). For people taking feminizing hormone therapy, testosterone suppression will lead to lower hemoglobin, hematocrit, and RBC counts that align with those seen in cisgender adult women. RBC indices stabilize by 6 months of initiating GAHT (36, 39, 46). There is a lack of published literature on longitudinal changes in hemoglobin, hematocrit, and RBC counts earlier than 6 months after initiating GAHT. Therefore, during the hormone initiation period, the hematology reference interval for SAAB should also be considered, as clinically indicated.
The 99th percentile upper reference limit (URL) is the recommended cutoff for the detection of myocardial injury using all cardiac troponin assays, including high-sensitivity cardiac troponin (hs-cTn). In healthy populations with random measurements, cisgender men have higher hs-cTn concentrations than cisgender women, making the 99th percentile URL for cisgender men a higher concentration compared with cisgender women (47). This trend is similar for transgender people, whereby transgender men prescribed testosterone have higher hs-cTn concentrations relative to transgender women, suggesting that sex hormones may influence cardiac physiology (23, 24). The clinical impact of sex-specific 99th percentile URLs in the assessment of acute myocardial infarction (AMI) has been debated, but prospective studies designed to measure long-term consequences of implementing sex-specific thresholds favor their use (48).
On a population level, sex-specific hs-cTn URLs likely improve outcomes and are being further assessed in clinical studies (49, 50). There have been no prospective clinical studies evaluating the influence of sex-specific 99th percentile URLs on long-term cardiac outcomes in transgender patients. However, in a small retrospective cohort evaluating classification of transgender patients based on use of sex-specific hs-cTn URLs, 3 patients with type 2 AMI (myocardial injury due to imbalance between oxygen supply and demand as opposed to coronary artery occlusion) had hs-cTn values that exceeded female but not male 99th percentile URLs. In 2 of these cases, the patients were transgender men, and results would have been falsely negative if using gender identity (male) but a true positive if using sex assigned at birth (SAAB; female). In contrast, the third reclassification was a transgender woman who would have been a true positive if using gender identity (female) but a false negative if using SAAB (male). No patients with type 1 AMI (blockage of the coronary arteries) were reclassified (51).
All four universal definitions of AMI include a rise and/or fall in cardiac troponin with at least one value exceeding the 99th percentile URL needed for the diagnosis of non-ST elevation myocardial infarction, implying that serial hs-cTn measurements to detect a change/delta are critical for diagnosis (52). Unless a specified rapid rule-out hs-cTn protocol is institutionally adopted, all patients presenting with signs and symptoms of AMI should receive serial measurements, and the delta hs-cTn concentration should be assessed and used to determine whether additional cardiac care is required (51). Overall, given the limited current evidence, we emphasize the importance of serial measurements of hs-cTn for the population receiving GAHT. If sex-specific hs-cTn URLs are applied institutionally, we provisionally recommend the use of the 99th percentile that aligns with affirmed gender, recognizing this is an area in need of future study. These recommendations are appropriate for both hs-cTnI and hs-cTnT.
The impact of sex hormones on kidney health and risk of chronic kidney disease (CKD) has been revealed through cross-sectional, epidemiologic, and animal studies (56). In the cisgender female population, estradiol shows protective effects on glomerular and tubular function, with earlier menarche or later menopause associated with lower risk of CKD (57, 58). In contrast, bilateral oophorectomy in premenopausal women is associated with a higher risk of developing CKD (59). The role of testosterone in kidney function is complex, with some conflicting studies in the literature (60).
Creatinine production is proportional to skeletal muscle mass such that the creatinine reference interval for cisgender adult men has a higher upper and lower limit of normal relative to cisgender women. Although testosterone is a known anabolic steroid that enhances skeletal muscle accrual, a systematic review and meta-analysis illustrated that the changes in creatinine concentration after initiating masculinizing or feminizing GAHT were variable (19). Combined, the analysis indicated that transgender men have a slight increase in creatinine concentration after initiating masculinizing therapy, but that transgender women show no significant change in creatinine concentration from feminizing therapy (33, 61). Interestingly, a study directly measuring the glomerular filtration rate (GFR) using iohexol clearance in transgender women and men showed an increase in measured GFR 3 months after starting feminizing therapy and no change in measured GFR 3 months after starting masculinizing therapy (62).
Clinically, the reference interval for creatinine is less relevant than the use of creatinine concentration in the context of calculating estimated GFR (eGFR), which is ideally calculated using the 2021 Chronic Kidney Disease Epidemiology Collaboration or similarly modern eGFR equation (63–65). These equations require input of 3 variables: age, sex, and creatinine concentration. The sex variable influences the numeric output of eGFR by approximately 30%, whereby a creatinine concentration of 1.5 mg/dL (132 µmol/L) for a 40-year-old adult would calculate an eGFR of 98 mL/min/1.73 m2 for an adult male (considered normal) and a value of 73 mL/min/1.73 m2 in an adult female (considered mildly decreased kidney function) (26). Factors other than hormones influence skeletal muscle mass, which can also result in significant differences between measured GFR and eGFR for individual cisgender people. For people receiving GAHT, there is no consensus on the use of SAAB or affirmed gender as most appropriate for eGFR calculations (65, 66). One study illustrated that the Chronic Kidney Disease Epidemiology Collaboration creatinine equation can overestimate eGFR by as much as 50% in transgender men when using the affirmed gender and 30% in transgender women when using SAAB (27).
Cystatin C is a skeletal muscle-mass independent analyte that is also used to estimate GFR. Slight differences in cystatin C have been observed between men and women, but the overall impact of these differences on population-derived eGFR equations is significantly less than that of creatinine-based eGFR equations (26). Cystatin C aligns with affirmed gender in those stably on GAHT, whereby use of masculinizing hormone therapy increases cystatin C and feminizing hormone therapy decreases cystatin C (25). These preliminary data support the use of affirmed gender in cystatin C-based eGFR equations. Alternatively, the most recent European Kidney Function Consortium cystatin C–based equation for eGFR does not include a sex variable (67, 68).
Sex is an influential variable in calculating eGFR, and laboratories should strive to provide educational activities that reinforce that muscle mass, sex hormone milieu, SAAB, and gender identity must be considered when interpreting creatinine-based eGFR results. For transgender people, eGFR should ideally be calculated using both male and female variables, although the ability to do this depends on the informatics capability of the LIS and EHR. If the eGFR calculated is 60 mL/min/1.73 m2 in someone on GAHT, additional markers of renal function, such as cystatin C, urine albumin to creatinine ratio (uACR), and direct GFR measurement, should be considered. In line with this, the 2024 Kidney Disease Improving Global Outcomes Chronic Kidney Disease guidance provided Grade 1C evidence using eGFRcr-cys (an eGFR equation incorporating both creatinine and cystatin C measurements) in clinical situations when eGFRcr is less accurate, and GFR estimation affects clinical decision-making (66).
The hypothalamic–pituitary–gonadal axis (HPGA) is the pathway that regulates sex hormones in humans (71, 72). In response to both environmental and internal cues, the hypothalamus secretes gonadotropin-releasing hormone (GnRH), which acts on the pituitary gland to stimulate the release of the gonadotropins: luteinizing hormone (LH) and follicle-stimulating hormone (FSH). In individuals with testes, LH promotes testosterone production. FSH, in conjunction with testosterone, prompts spermatogenesis. For individuals with ovaries, FSH and LH together regulate the menstrual cycle through estradiol and progesterone production. The axis is sensitive to negative feedback, whereby, in general, increased concentrations of testosterone and estradiol (whether endogenous or exogenous) lead to the downregulation of GnRH, LH, and FSH, facilitated by kisspeptin-expressing neurons. GAHT impacts the HPGA by suppressing endogenous hormone expression. The overall effect includes changes to the concentrations of estradiol and testosterone, as well as other hormones and hormone metabolites related to the HPGA. Clinical guidelines related to GAHT for transgender people recommend measuring estradiol and testosterone, although there is debate on the frequency of monitoring and target concentrations (3, 5)
Estradiol therapy suppresses GnRH and gonadotropins, with subsequent suppression of testosterone. When prescribed as monotherapy, injectable estradiol can be sufficient to suppress endogenous testosterone, whereas oral and transdermal estradiol monotherapy are often insufficient (16, 73). Consequently, transgender women using these forms of estrogen are often coprescribed antiandrogens if they have not had an orchiectomy (3). In the United States, the most common antiandrogen is spironolactone, whereas CPA is used outside of the United States. GnRH agonists can also be prescribed as antiandrogens, but high cost limits their use. Spironolactone and CPA impart their antiandrogenic activities through different mechanisms (16). Spironolactone primarily acts as an androgen receptor antagonist and only minimally decreases testosterone concentration. Conversely, CPA inhibits GnRH secretion, leading to additional HPGA suppression and significant testosterone concentration reduction. Finasteride is an antiandrogen medication that inhibits 5α-reductase and prevents the conversion of testosterone to dihydrotestosterone. While finasteride is sometimes prescribed to aid in feminization, routine use (except as therapy for other indications such as androgenic alopecia) is not recommended (3). Overall, antiandrogen use is an important factor to consider when evaluating laboratory results for transgender women.
The Endocrine Society and WPATH recommend monitoring estradiol and testosterone every 3 months during the first year of feminizing GAHT or with dose changes until stable dosing is reached, following which sex hormones should be monitored annually or biannually (3, 5). Estradiol and testosterone should be interpreted using a different reference interval than the menstrual cycle phase–specific ones that are used for cisgender women (Table 2) (74). For transgender women, current guidance based on expert opinion recommends that estradiol be maintained in a range of 100 to 200 pg/mL (367–734 pmol/L) (5). However, this interval does not reflect empirical evidence of an adequate therapeutic range, with multiple studies supporting a range wider than 100 to 200 pg/mL (367–734 pmol/L) (20). In addition, estradiol concentrations must be interpreted in the context of key preanalytical factors, such as therapeutic regimen, antiandrogen therapy, mode of hormone administration, time since the last dose, and individualized goals of feminizing therapy (74). More studies are needed to determine expected, toxic, and/or sufficient estradiol concentrations in populations prescribed feminizing therapy. Use of exogenous estradiol is associated with a slightly increased absolute risk of thromboembolism (relative to baseline) and should be evaluated against the goals of therapy using combined informed consent to guide the therapeutic regimen (75, 76).
Clinical guidelines state that for transgender women, total testosterone should be suppressed to <50 ng/dL (<1.7 nmol/L) (5). Circulating testosterone concentrations depend strongly on antiandrogen use and history of orchiectomy. Patients prescribed CPA or who are postorchiectomy typically have testosterone values that approximate concentrations observed in cisgender women, who generally have a total testosterone reference interval of <50 ng/dL (<1.7 nmol/L). Patients prescribed spironolactone may not suppress testosterone to concentrations observed in cisgender women, especially if estradiol concentrations are suboptimal or there is inconsistency with estradiol dosing (16, 17). Because spironolactone primarily works by blocking androgen receptors, desired feminization may be achieved even with relatively higher testosterone concentrations. Feminization goals are personalized and can be accomplished in the setting of testosterone above the cisgender female range (76).
Patient factors that can impact estradiol and testosterone concentrations include hormone formulation, mode of administration, frequency of dosing, time since the last dose, use of antiandrogen (for feminizing GAHT), and individualized goals of GAHT (Table 3). Estradiol and testosterone immunoassay measurements are susceptible to interferences stemming from the preanalytical and analytical phases of testing (79). These factors are not unique to GAHT but can complicate the interpretation of hormone concentrations. Measurement error or assay interference should be considered if reported hormone concentrations are unexpectedly high or low. Immunoassays for estradiol and testosterone may lack the analytical sensitivity to measure low hormone concentrations. Mass spectrometry–based confirmatory methods should be considered in cases where immunoassay measurements yield unexpected results or where determination of hormone concentrations below immunoassay analytical sensitivity is clinically indicated (88, 89).
Circulating concentrations of total testosterone are affected by concentrations of sex hormone–binding globulin (SHBG). A variety of clinical conditions and medications are associated with abnormal concentrations of SHBG, including thyroid disorders, polycystic ovarian syndrome, insulin resistance, and exogenous hormones (94). Measurement of free testosterone may be useful when total testosterone concentrations yield confusing or unexpected results (95, 96). In transgender men, cisgender male reference intervals for free testosterone can be used for interpretation (18). There is currently insufficient evidence to guide the interpretation of free testosterone concentrations in transgender women.
| Factor | Potential effects | Actions/gaps in knowledge |
| Formulation and dosing schedule of estradiol or testosterone (79) | Different formulations (oral, parenteral, topical) have different pharmacokinetics. Interpretation of hormone concentrations is influenced by these variables. | More data are needed to determine the impact of hormone formulations on target concentrations, desired clinical effects, and potential adverse effects of estradiol and testosterone for gender-affirming care. |
| Draw site contamination by topical hormone preparations, especially gel (80–84) | Erroneous, supratherapeutic concentrations | Counsel the patient to avoid topical steroid application near phlebotomy draw sites and/or draw blood in the contralateral site from gel application. Can measure FSH and LH to help interpret (will be suppressed if actual serum/plasma concentrations are supraphysiological in a sustained manner). |
| Cross-reactivity of estradiol and testosterone immunoassays (79, 85) | Variable across different marketed assays. Estrone (from oral estradiol formulations) cross-reacts with some estradiol immunoassays (86, 87). | Cross-reactivity should be considered as a possible factor impacting immunoassay results. Mass spectrometry-based assays may be useful in some clinical circumstances (88, 89). |
| Biotin interference with immunoassays (90) | Competitive immunoassays for estradiol and testosterone using biotinylated reagents may be vulnerable to falsely elevated values from biotin in those taking high-dose biotin supplements (91). | Some marketed immunoassays using biotinylated reagents have been reformulated to minimize biotin interference (92, 93). Limited data are currently available for biotin interference in hormone assays |
SHBG is useful for the calculation of free testosterone using mathematical models such as the Vermeulen equation or other calculators (95, 96). Although routine measurement of SHBG is not recommended by WPATH or the Endocrine Society (3, 5), estradiol stimulates SHBG; therefore, SHBG concentrations often increase in people taking feminizing hormone therapy and decrease in people taking masculinizing therapy (17, 18, 29). This is most pronounced with oral estradiol treatment (17, 29). The reference interval for SHBG for transgender women, as determined in a single study, spanned a wider concentration range than the corresponding reference intervals for either cisgender women or cisgender men (17). The reference interval for SHBG in transgender men most closely approximated the reference interval for cisgender men (18). However, as the primary use of SHBG is to calculate free testosterone, these changes are clinically relevant in their influence on testosterone interpretation.
Measurement of LH and FSH may be clinically indicated in instances where estradiol or testosterone concentrations are unexpectedly high or low and/or when phenotypic effects are insufficient relative to goals of GAHT (97). LH and FSH can provide context for estradiol or testosterone values measured at a single time point (i.e., is the HPGA suppressed, balanced, or activated?) and can be trended over time as a measure of hormone stability. There are few data investigating the exact impact of feminizing or masculinizing therapy on FSH and LH, but changes likely depend on surgical history, antiandrogen use, progestogen use, and the temporal relationship between estradiol or testosterone administration and the response to exogenous hormone therapy (30).
Guidance documents from the Endocrine Society and WPATH do not suggest routinely monitoring LH and FSH in adults prescribed GAHT (3, 5). There have been studies that support LH suppression as a correlate to a positive body image and quality of sex life (98) and others indicating that adequate feminizing therapy is usually accompanied by an LH concentration less than 1.0 mIU/mL (99). In cisgender people, elevated FSH has been shown to predict bone loss (100). Understanding the relationship between GAHT and LH and FSH concentration in transgender people is an important area of future study.
Studies of progesterone in those taking GAHT have been largely limited to the influence of progesterone on pregnancy in transgender men and not on the phenotypic influence of progesterone on physiological processes in transgender men or women. For transgender men using masculinizing hormones, use of testosterone should inhibit progesterone production (18). However, since ovulation may still spontaneously occur, progesterone may be transiently detected (31). Early follicular phase reference intervals applied to cisgender women can be used as a guide to ensure adequate progesterone suppression in transgender men, if clinically indicated (18).
Transgender women may be coprescribed progesterone with estradiol to enhance feminization (particularly breast development) or improve other health aspects such as sleep or libido (32, 101, 102). There is an absence of data to indicate what concentrations of progesterone would be ideal as a treatment goal for those receiving feminizing GAHT, but a recent study indicated that patient satisfaction may be improved by coprescription of progesterone (32).
Changes in dehydroepiandrosterone sulfate (DHEAS) and anti-Müllerian hormone concentrations from GAHT appear to be complex, and there is insufficient data indicating how masculinizing or feminizing therapy affects these analytes. For DHEAS, the concentration ranges observed in transgender women and men more closely parallel the reference intervals associated with SAAB as opposed to affirmed gender (17, 18, 103). The impact of GAHT on adrenal hormones such as DHEAS may be multifaceted and is incompletely understood (104). The interpretation of anti-Müllerian hormone as a marker of ovarian reserve in transgender men receiving testosterone is also an area of evolving study (105).
Interpretation of lipid parameters is largely independent of sex, with clinical guidelines applying the same treatment thresholds for most lipid values regardless of gender (106). The primary exception is HDL cholesterol (HDL-C), which historically has had higher optimal target concentrations in females (>50 mg/dL [>1.3 mmol/L] for female; >40 mg/dL [>1.0 mmol/L] for males). In transgender patients receiving GAHT, lipoprotein concentrations often shift in the direction of the affirmed gender (33). Estrogen therapy in transgender women may increase HDL-C and slightly decrease LDL cholesterol and triglycerides. Conversely, testosterone therapy in transgender men may reduce HDL-C and slightly increase LDL cholesterol and triglycerides (34, 35). These changes generally stabilize within 6 to 12 months of initiating therapy (33, 39, 46).
Despite hormone-related effects on lipoprotein metabolism, clinical management should focus on target concentrations and overall cardiovascular risk, rather than sex-based reference intervals. Routine monitoring of lipoproteins is recommended, particularly during the early stages of GAHT, to guide individualized risk assessment and treatment planning. Specific guidance on the timing or frequency of monitoring lipid measurements is lacking, but most changes in response to hormone therapy will take at least several weeks to significantly change. There is currently no consensus on how to utilize lipid markers to estimate long-term cardiovascular risk in the population receiving GAHT; this is an area of active inquiry with a need for future research (107, 108).
Prolactin production by the anterior pituitary is stimulated by estrogen. Hyperprolactinemia is one of the most common disorders of the hypothalamic–pituitary axis and is associated with hypogonadism in both men and women (111). Upper reference limits for prolactin are higher in cisgender women relative to cisgender men, but there is significant overlap between these sex-specific reference intervals. Multiple reports suggest that feminizing therapy regimens using estradiol and CPA modestly increase prolactin from baseline (38, 112–115). There is evidence that CPA is the causative factor for the observed increase (112, 113).
The 2017 Endocrine Society guidelines recommend routine monitoring of prolactin to screen for hyperprolactinemia in those receiving GAHT (5), but there is insufficient evidence linking estradiol therapy itself (as opposed to CPA) with an increased risk of hyperprolactinemia or prolactinoma (20). CPA is not approved for clinical use in the United States; therefore, the antiandrogen used needs to be considered. While there is no guidance for what concentration of prolactin is expected in transgender women, in the rarely reported instances of symptomatic hyperprolactinemia, prolactin concentrations were several-fold higher than the upper limit of normal for cisgender women (116). Based on available evidence, cisgender female reference intervals for prolactin can be used for those receiving feminizing GAHT. Routine prolactin monitoring is not recommended for individuals prescribed GAHT unless they are experiencing signs and symptoms of hyperprolactinemia or prolactinoma (40).
There is a global deficiency in cervical cancer screening. Within the United States, underscreening is particularly pronounced in the transgender population (117, 118). Pap testing has traditionally been the mainstay of cervical cancer screening. There are, however, some challenges to Pap testing in transgender men, including a high rate of unsatisfactory Pap tests (119) as well as cytologic changes from long-term testosterone therapy. Cervical and vaginal epithelial changes from masculinizing GAHT can mimic the effects of human papillomavirus (HPV) infection, making it difficult to distinguish HPV-related changes from hormone-related tissue atrophy (120–122).
HPV primary screening is an effective approach to screen for precancerous cervical lesions and to prevent the development of cervical cancer (123, 124). This screening method relies on the detection of HPV nucleic acid sequences, which can be detected from vaginal specimens and therefore does not initially require collection of a cervical specimen. This contrasts with the Pap test, which requires collection of a cervical specimen for cytologic analysis (123). The enhanced negative predictive value of HPV primary screening allows for approximately 90% of screening individuals to be triaged without collection of a cervical specimen.
Vaginal specimens, which involve superficial insertion and rotation of a swab in the vaginal canal, are uniquely positioned for self-collection with or without the need for a clinical encounter. Most people are comfortable with self-collection of vaginal specimens and can perform the collection process in a nonclinical setting, like at home or in a private area at a clinic or health fair (125). Additionally, multiple studies have illustrated a preference for vaginal self-collection among transgender people (126,127). HPV primary screening with the option for vaginal swab self-collection would be ideal for transgender people with a cervix (128, 129).
Prostate-specific antigen (PSA) plays a role in both the diagnosis and monitoring of prostate cancer. Generally, prostate cancer screening for transgender adults should be performed in accordance with local guidelines (3). Considering that transgender women retain their prostate even following orchiectomy and/or vaginoplasty, clinical recommendations for prostate cancer screening should be followed. Currently, PSA values for transgender women are evaluated using cisgender male interpretive ranges. While there is a paucity of data evaluating the impact of feminizing hormone therapy on PSA concentrations, there is evidence that transgender women have significantly lower baseline PSA values relative to cisgender men, and a PSA cutoff of 4.0 ng/mL may not have appropriate sensitivity to screen for prostate cancer in transgender women prescribed estradiol (130). A lower PSA threshold of 1.0 ng/mL has been proposed for transgender women (131), but the caveats for PSA as a cancer screening marker still apply (132). This is an area in need of future research, including the study of long-term outcomes. Interpreting prostate biopsies should follow guidelines for cisgender men (130, 133). Transgender men do not have prostates; therefore, PSA is not detectable in this population, and testing is not clinically indicated.
Optimal specimen types to screen for certain sexually transmitted genital infections differ between cisgender men and women, whereby mid-stream first-void urine is the specimen of choice for people with a penis, and vaginal swabs are the specimen of choice for those without (13). There are currently no studies identifying the optimal specimen type in transgender men and women prescribed GAHT regardless of genital surgery, but expert consensus suggests people should be sampled at anatomic sites about which they have concerns of exposures (134–137). Ensuring flexibility in the laboratory operational design, whereby vaginal swabs from men and urine samples from women are acceptable sample types, is important to ensure optimal access to testing and timely result reporting across genders (13, 129). Future studies should determine the optimal specimen types from transgender people. In addition, some assays do not have US Food and Drug Administration (FDA) approval for some specimen types, necessitating laboratory-developed test validations. An expansion of FDA-approved assays for multiple specimen types would be beneficial across patient populations.
The 2023 change in FDA guidance toward a gender-neutral and risk-based donor history questionnaire has improved several aspects of donor eligibility assessment (138). For instance, since all potential donors are asked about pregnancy history regardless of gender identity, the residual risk of transfusion-related acute lung injury from transgender men donating plasma is considered minimal (139). However, important clinical and operational considerations remain that may affect the safety of both transgender donors and transfusion recipients. These include limitations in existing information systems, differences in physiologic parameters based on sex and hormone therapy, and gaps in standardized approaches to donor and recipient classification.
A persistent limitation in transfusion medicine is the inability of most blood establishment information systems to separately record gender identity and SAAB. Per FDA guidance, gender may be self-identified and self-reported but must be limited to the binary options of male or female (138). Consequently, most blood centers do not offer an option for nonbinary donors who do not identify as either gender (140).
Donor eligibility criteria are traditionally based on sex-specific physiologic parameters, including hemoglobin and hematocrit reference intervals. Recording both gender identity and SAAB as distinct data points would allow for more accurate donor evaluation and safer collections; however, determining gender-neutral hemoglobin ranges or donation intervals that err on the side of safety could potentially eliminate the need to collect both gender and SAAB and make it possible to allow a wider range of gender options (140–142). The latter approach would also benefit donation practices in hypogonadal cisgender people.
For transgender recipients of blood products, accurate SAAB documentation remains essential for blood product selection, particularly in emergencies. When the recipient’s ABO type is unknown, group O RBCs are administered. Because D-negative units are a limited resource, they are prioritized for patients with potential for pregnancy to reduce the risk of D alloimmunization and hemolytic disease of the fetus and newborn. In emergent settings, reproductive history and gender identity may not be available. Institutional policies often address this uncertainty by assuming reproductive potential in cisgender women up to a defined age threshold, which may inadvertently exclude some patients or lead to inconsistent application of safety precautions. Rh-positive blood products should also be avoided for transgender men who retain a uterus to prevent alloimmunization and potential complications in future pregnancies (143). Conversely, transgender women who were assigned male at birth do not share these reproductive risks and can safely receive Rh-positive blood if needed, provided that this information is available for blood bank staff to make the appropriate substitution according to institutional standard operating procedures.
Medicolegal death investigations lack standardized guidance on documenting gender identity, which often results in inaccurate or absent reporting of gender identity in official records (144, 145). Inconsistent or absent data on gender identity makes research on transgender and nonbinary decedents challenging and affects the accuracy of mortality surveillance, especially for deaths from violence or suicide, which can make it difficult to identify health disparities and patterns of violence (146, 147).
Forensic pathologists should document both the legal and chosen/correct name and gender, with the legal name being used for legal or administrative purposes and the chosen/correct name used whenever possible. Gender identity should be verified using medical and legal records, chosen family, or other designated decision makers, and should not be limited to family of origin (144). When discrepancies occur, reports can include clarifying statements such as “The decedent identified as a transgender man and used the name [affirmed name].”
Anatomic findings should be described neutrally using inclusive terminology such as SAAB instead of biological sex and phenotypic male/female genitalia instead of gendered labels. Pathologists should note evidence of gender-affirming care (e.g., surgical scars, implants, hormonal changes) without speculation (144). Despite frequently appearing in forensic pathology textbooks, terminology such as crossdresser or transvestite is not synonymous with transgender identity. These terms are outdated and inaccurate and should be avoided (144).
Over half of transgender and gender-diverse decedents in Oregon had incorrect gender identity on death certificates, creating discordance between medical examiner data and vital records (145). Death certificates should reflect affirmed identity whenever possible, with the narrative and investigative reports providing clarification when legal requirements prevent this.
Training initiatives demonstrate that SOGI data can be collected accurately with structured education and leadership support (148). Scene investigators can also facilitate accurate gender-identity reporting. Several jurisdictions now have laws regarding gender identity after death, including California (149), New York City (150), New Jersey (151), Colorado (152), and the District of Columbia (153).
GAHT and/or surgical procedures impact secondary sexual characteristics and organ histology. This section summarizes tissue-based changes associated with GAHT or gender-affirming surgeries. As part of the examination of the resected tissues, the pathologist will evaluate and document these findings. Other clinical scenarios exist where a pathologist may examine tissue specimens from transgender individuals without knowledge of their transgender status or hormone therapy history. For example, pathologists may receive prostate gland biopsies from transgender women or oophorectomy specimens from transgender men for reasons unrelated to the individual’s gender affirmation. When gender-affirming surgery is preceded by long periods of GAHT, hormone-related histologic changes are seen (14, 15).
For transgender men undergoing reduction mammoplasty, specific guidelines for the gross examination and subsequent tissue submission of mastectomy specimens have not been standardized. There is currently no evidence to suggest that GAHT increases the incidence of breast cancer in transgender men (154). Accordingly, local institutional protocols for reduction mammoplasty specimens from cisgender women may be followed, with additional tissue evaluated if atypical proliferations are identified on initial examination. Documenting the size and weight of the product of a mastectomy, along with what exactly was removed, is important since surgery does not necessarily remove all identifiable breast tissue. There is a lower incidence of breast cancer in transgender men receiving testosterone than in cisgender women. However, there is a higher risk of breast cancer in transgender women receiving estradiol compared with cisgender men (155). Long-term follow-up studies are needed to better understand the risk of breast cancer in this population; thus, future studies may facilitate refinement of pathology procedures.
Documenting the inclusion of the cervix and fallopian tubes in hysterectomy specimens from transgender men is important for future cancer screening plans, including cervical cancer screening and ovarian-related oncology (e.g., BRCA mutation or family diagnosis of ovarian cancer), respectively.
Orchiectomy specimens from transgender women can be serially sectioned for the identification of any grossly identifiable lesion. A spermatic cord en face margin and 2 or 3 cross-sections, including both rete testis/epididymis are submitted for histopathologic examination (156).
In hysterectomy specimens from transgender men on long-term masculinizing GAHT, the endometrium may show expanded endometrial stroma with endometrial glandular atrophy (157), areas with decidua-like changes and occasional vacuolated cells, and glandular paucity (Fig. 1A) (158). Rarely, endometrial polyps showing hyperplasia without atypia are seen (159). Changes in cervical epithelium from masculinizing therapy with testosterone include ectocervical epithelial atrophy, transitional cell metaplasia (Fig. 1B) (158), and, rarely, prostate-type glands at the base of ectocervical epithelium (160). From salpingo-oophorectomy specimens, periadnexal tissue may show the presence of virilized mesonephric duct remnants (160). Changes in ovaries from masculinizing therapy include large follicular cysts lined by nonluteinized granulosa cells (161), higher follicular density than typical for chronologic age (158), thickening of the tunica albuginea, and stromal hyperplasia (Fig. 1C) (161). Testosterone therapy induces histologic changes in vaginal mucosa that include epithelial atrophy, transitional cell metaplasia, and prostate-type glands at the base of the ectocervical epithelium (Fig. 1D) (162). In mastectomy specimens from transgender men, histologic changes can include lobular atrophy with fewer lobules, gynecomastoid changes (163), stromal fibrosis, fibrocystic changes, and microcalcifications (Fig. 2) (164). Table 4 summarizes histologic changes seen in tissues from long-term masculinizing GAHT.
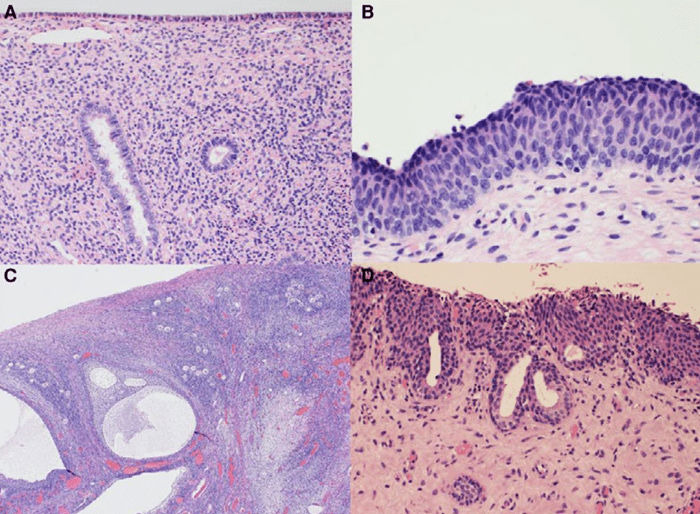
Fig. 1. Androgen-related histologic changes seen in hysterectomy and vaginectomy specimens. (A), Specimens feature plump endometrial stromal cells with ample cytoplasm and sparse inactive small glands; (B), Ectocervical epithelium resembles urinary bladder epithelium with nuclear grooves, umbrella-like cells on the surface, and a virtual absence of the cuboidal palisaded basal layer; (C), Ovaries exhibit large cortical follicular cysts lined by nonluteinized granulosa cells, accompanied by a relatively higher number of primordial follicles for the individual’s age; (D), Vaginal mucosa is typically atrophic with transitional cell metaplasia and benign prostate-like glands at the epithelial–stromal junction.
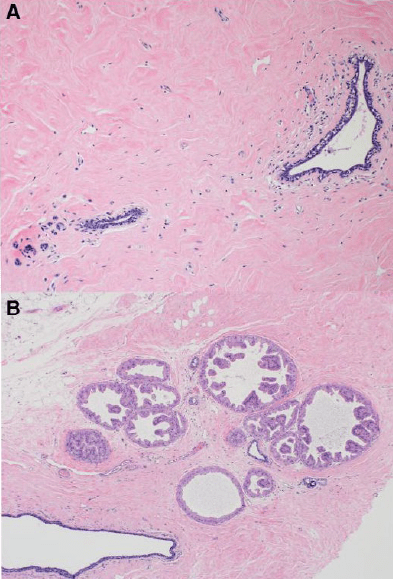
Fig. 2. Androgen-related histologic changes seen in mastectomy specimens. (A), Specimens feature lobular atrophy with atrophic ductal epithelium and stromal hyalinization/fibrosis; (B), Fibrocystic changes with apocrine metaplasia and calcification could also be present.
Table 4. Histologic changes seen in tissues in those with gender-affirming gonadectomy preceded by long-term gender-affirming masculinizing hormone therapy.
| Procedure | Tissue received | Histologic changes |
| Hysterectomy (see Fig. 1A and B) | Endometrium | • Expanded endometrial stroma with endometrial glandular atrophy (157) • Areas with decidua-like changes and occasional vacuolated cells (158) • Glandular paucity (158) • Rarely, endometrial polyp, hyperplasia without atypia (159) |
| Cervical epithelium | • Ectocervical epithelial atrophya (158) • Transitional cell metaplasiaa (158) • Rarely, prostate-type glands (prostatic metaplasia) at the base of ectocervical epitheliumb (160) |
|
| Salpingo-oophorectomy (see Fig. 1C) | Periadnexal tissue | • Periadnexal virilized mesonephric duct remnants (160) |
| Ovaries | •Large follicular cysts lined by nonluteinized granulosa cells (161). Follicular density (primordial, intermediate, and primary follicular count per square mm) is higher than expected for the given age (158) •Thickening of the tunica albuginea (161) •Stromal hyperplasia (161) | |
| Vaginectomy (see Fig. 1D) | Vagina | •Epithelial atrophya (162) •Transitional cell metaplasiaa (162) •Prostate-type glands (prostatic metaplasia) at the base of ectocervical epitheliumb (162) |
| Mastectomy, reduction mammoplasty (see Fig. 2A and B) | Breast | •Lobular atrophy, fewer lobules (163) •Gynecomastoid change (atrophic duct epithelium and peripheral hyalinization/fibrosis) (163) •Stromal fibrosis (164) •Fibrocystic changes (164) •Microcalcifications (164) •Virtually every proliferative and neoplastic lesion described in cisgender women has been observed in breast specimens from transgender men receiving testosterone (14). |
a Differential diagnosis of epithelial atrophy and transitional cell metaplasia of the ectocervix and vagina. Special attention is given not to overdiagnose these lesions as high-grade intraepithelial lesions. Umbrella-like cells could be seen on the surface, and these cells feature nuclear grooves. P16 immunohistochemical staining shows patchy, weak positive staining.
b Differential diagnosis of prostate-like glands (prostatic metaplasia). These cells are positive for NKX3.1, PSA, and p501s. They exhibit no nuclear atypia. Special attention must be given to not mistake prostate-type glands in the cervix for dysplasia or glandular proliferative abnormalities.

Fig. 3. Estrogen-related histologic changes seen in orchiectomy and penectomy specimens. (A), There is testicular atrophy with increased stromal/basement membrane fibrosis, reduction of Leydig cell numbers, and Sertoli cell cytoplasmic vacuolization; (B), Typically, penile urethral epithelium undergoes squamous cell metaplasia.
Table 5. Histologic changes seen in tissues in those with gender-affirming gonadectomy preceded by long-term gender-affirming feminizing hormone therapy.
| Procedure | Tissue received | Changes |
| Orchiectomy (see Fig. 3A) | Testis | • Increased fibrosis (15) |
| • Testicular atrophy (156) | ||
| • Reduced Leydig cell numbers, which are responsible for testosterone production (15) | ||
| • Sertoli cell cytoplasmic vacuolization (15) | ||
| Penectomy (see Fig. 3B) | Penis | • Squamous cell metaplasia of the penile urethral epithelium (165) |
| Bone trabeculae | Bone marrow biopsy | • Suppression of bone turnover without bone volume loss (166) |
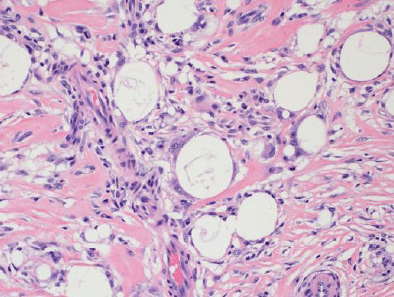
Gender-affirming surgery with or without prior GAHT may generate tissues submitted to pathology with nonhormone-related changes. Complications of masculinizing surgeries may include urethral stenosis, fistulae, sinus tracts, and abscess formation (167). Tissues resulting from the gender-affirming surgery itself or managing its complications are handled in the pathology laboratory as per the local protocols similar to those received from cisgender persons. Some augmentation procedures can be associated with foreign body reactions to exogenous material injections and silicone implants (Fig. 4).
Informatics has a significant impact on how laboratory medicine and pathology can provide affirming care for the transgender population. As with the general public, healthcare professionals may not be familiar with terminology and concepts related to sex and gender (168). As highlighted in the following discussion, the capabilities of software used in healthcare, including LIS systems for clinical laboratories, are also highly variable with respect to functionality related to gender-diverse patient identity and who has permission to change SOGI status within the EHR.
Patient names in legal documents, date of birth, and medical record numbers are primary patient identifiers within the healthcare setting, including insurance billing and reporting of information to public health authorities (168–171). Transgender patients may adopt a different name than their birth name to align with their gender identity. Transgender patients may elect to change their name on identity documents and/or in the medical record. In the healthcare setting, a change of patient name in legal documents can follow patient identification policies that apply in other situations, such as marital name changes. However, given that these changes require effort and expense, the birth name may still be the name in the medical record.
Some healthcare organizations have adopted a trauma-informed option that allows patients to provide a chosen/correct name that signifies how the patient wants to be addressed, including in waiting areas (172). Use of the chosen/correct name to identify patients in the healthcare setting is beneficial for all patients and may be especially important to transgender patients to avoid use of a name with which they no longer identify. There are challenges that need to be reviewed and managed in healthcare environments to ensure the proper use of the chosen/correct name and identification (170). Common practical challenges include display and visibility of the chosen/correct name on specimen labels and computer displays for the EHR and LIS. Hospital and clinical laboratory policies and procedures should specify whether the legal name is required for certain activities, such as collecting laboratory specimens, or when a chosen/correct name may substitute.
Functionality for SOGI data elements in records, commonly known as SOGI fields, has become available in some EHRs and LISs in recent years (170, 171, 173–176). SOGI fields include options for patients to voluntarily provide sexual orientation, SAAB, gender identity, and pronouns (e.g., he/him/his, she/her/hers, they/them/theirs). More advanced functionality includes fields that document current use of GAHT, history of gender-affirming surgeries, and organ inventories. Information in the SOGI fields can facilitate optimal interpretation of laboratory tests and analysis of anatomic pathology specimens (11, 170, 177). Some institutions do not utilize SOGI fields for a variety of reasons, including the absence of SOGI functionality in the specific EHR for the institution, lack of informatics resources to implement this functionality, or restriction by laws or policies related to gender identity (178). Table 6 summarizes applications and potential challenges with the use of SOGI fields in laboratory medicine and pathology.
| SOGI-related data | Applications and uses relevant to pathology | Potential limitations and risks |
| Patient name (legal documents) | Official name used throughout medical documentation and billing, including patient identification bands/labels and laboratory specimen labels | May differ from the chosen/correct nameRisk of using a name that patient no longer identifies with |
| Chosen/correct name | Name by which patient wants to be addressed in medical settings, including waiting rooms (including phlebotomy), inpatient units, and procedural areas; ideally, it is easily visible within EHR and LIS. | Some healthcare policies and practices may require the use of a legal nameChosen/correct name may either be absent or not easily visible on specimen labels, EHR, or LIS screens, depending on informatics capability and institutional practice. |
| SAAB | Health maintenance alerts and laboratory testing logic for which knowledge of SAAB drives clinical decision-making | May disclose gender identity even if irrelevant to a specific encounter |
| Pronouns | Guidance on how to refer to a patient when speaking to others or in medical documentation | May disclose gender identity even if irrelevant to a specific encounter |
| Gender identity | Specific reference intervals, result comments, or interpretation applied to anatomic and clinical pathology specimens and tests for which gender identity provides important context | May disclose gender identity even if irrelevant to a specific encounter |
| Gender-affirming hormone or surgeries (if available as SOGI fields, such as flags for gender-affirming hormone or organ inventories) | Specific reference intervals, interpretive comments, or interpretation applied to laboratory tests or anatomic pathology specimens potentially impacted by gender-affirming hormones or surgeries | Functionality not widely used in EHRs |
For those institutions that have implemented SOGI functionality in the EHR, published literature on the extent of patient use of these SOGI fields varies, with data coming mainly from larger institutions (176, 179, 180). Typical rates for patient volunteering of SOGI information, such as gender identity, SAAB, and sexual orientation, are approximately 20% to 30% at larger institutions that have implemented SOGI functionality, although rates can be higher for the gender-diverse patient population. Institutional factors that impact clinical use of SOGI fields include EHR capability, decisions to implement specific SOGI functionality, and workflows for the collection of SOGI data. Patient factors include health literacy, understanding of SOGI terminology, use of EHR patient portals (if these allow SOGI data input), and comfort with providing the information (168, 176, 179–181). SOGI information can present risks to patient privacy and confidentiality if viewed by individuals who can access the patient record (171, 182–186). EHR regulations in the United States around SOGI information include the privacy, security, and confidentiality considerations that apply to all sensitive health data; however, like all electronic health data, there are security risks to including this information in the EHR (187, 188).
Pathology personnel can facilitate optimal use of SOGI-related demographic data. There are limited available data on the state of cultural competency and the need for training clinical laboratory personnel (169, 189). But at a high level, pathology and informatics staff can help evaluate the EHR, LIS, and middleware software for SOGI functionality and how it might impact pathology results (170). For some institutions, the EHR and LIS have differences in SOGI functionality, especially if the EHR and LIS are from different vendors. Thus, even if SOGI information is available in the EHR, the LIS or laboratory middleware software may not be capable of utilizing that information. In that scenario, a clinical laboratory that assigns reference intervals in the LIS will be unable to incorporate SOGI logic. Additionally, even if an institutional EHR and LIS have SOGI functionality, the SOGI data fields may be inaccessible to reference laboratories that analyze specimens from that institution.
The legal sex marker in the EHR and administrative documents has traditionally been the main sex identifier used in healthcare (173). Legal sex is typically displayed together with name and date of birth on patient identification labels and medical record documentation. For laboratory tests that have sex-specific reference intervals or calculations, legal sex impacts which intervals or calculations are used for interpretation and subsequent medical decision-making (180, 190–192). Institutional protocols and EHR alerts may also utilize logic based on this documented sex. For example, health maintenance and decision support algorithms in the EHR may utilize legal sex in the logic for sex-specific reminders and alerts for cervical or prostate cancer screening, pregnancy testing prior to surgery, mammography, and cardiovascular risk assessment.
Some transgender patients elect to change their gender marker on identity documents, a process influenced by laws and policies at international, national, and local levels (193, 194). Healthcare organizations have varying policies for how to change legal sex within the medical record; prior change of 1 or more identity documents may be required. Within the United States and its territories, the ability to change the gender marker on identity documents is mainly subject to federal and state laws. Some states within the United States do not allow any change of the gender designation marker on motor vehicle and other state identity documents, while other states permit this change (194).
Change of legal sex within the medical record may include a change from male to female or female to male or to another sex marker, such as unknown (U), *, X, or nonbinary (if institutional practice offers these options) (180, 195, 196). A change of legal sex in the EHR has downstream consequences in terms of sex-specific reference intervals, billing for procedures that have coding based on a binary sex classification (e.g., pregnancy screening, PSA testing), healthcare maintenance alerts, and decision support logic. One important consideration is that changes in EHR legal sex and/or gender identity markers can occur even for those not receiving GAHT or who discontinue or pause GAHT at some point. This adds a layer of complexity to interpreting laboratory tests that have sex-specific reference intervals. Consider the situation where a transgender man has gone through the process to change his legal sex in the EHR to male. All logic for sex-specific reference intervals, health maintenance alerts, and procedural billing will use male as the legal sex. In the absence of EHR logic that recognizes the patient as transgender, alerts and decisions based on a female SAAB would be missed. These include pregnancy testing prior to procedures, health maintenance alerts for cervical cancer screening or mammography, and use of Rh-negative blood for emergency administration. In this scenario, a SOGI field for SAAB would be beneficial and practical.
Tissue specimens from transgender patients may be misidentified when the legal sex does not match the expectation (e.g., prostate specimen from a transgender woman who has changed legal sex to female; cervical biopsy from a transgender man who has changed legal sex to male) (170, 191, 192). There are also people with nonbinary or similar gender identities. As mentioned previously, some EHRs allow for options like *, X, and nonbinary in the legal sex field, a scenario that can create challenges with sex-specific reference range assignment, including potential safety issues, if no reference interval gets applied to specific testing in the event that legal sex is something other than male or female (195).
There are multiple approaches for reporting reference intervals/ranges that may be impacted by GAHT (Fig. 5 and Table 7). There is a relatively short list of common laboratory tests significantly impacted by GAHT based on current evidence (Table 2). Of common nonhormonal laboratory tests, hemoglobin/hematocrit/RBC count demonstrates the clearest shift toward affirmed gender for those stably receiving either feminizing or masculinizing hormone therapy.
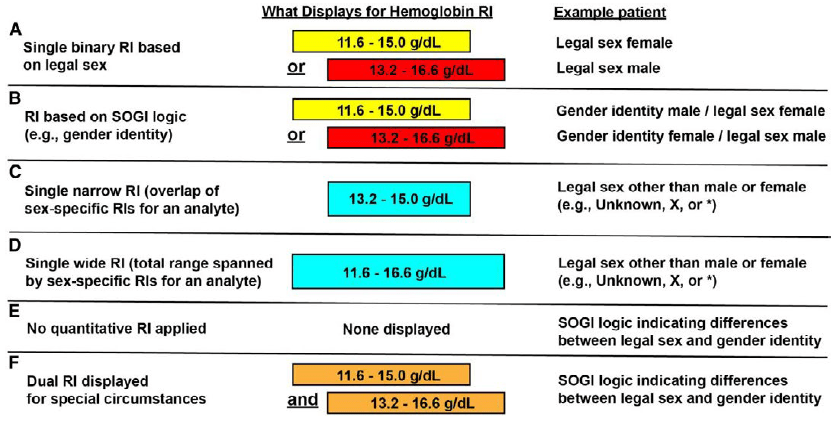
Table 7. Approaches for handling reference ranges/intervals for tests with sex-specific reference intervals.
| RIa used | Advantages | Disadvantages/challenges |
| Single binary RI based on legal sex | • Simple and familiar (typically the default approach for sex-specific RIs) | • A subset of transgender patients change their legal sex. • Legal sex is not available in the EHR for some patients. • Legal sex may have options other than male or female (e.g., unknown, X, *). |
| RI based on SOGI logic (e.g., gender identity) | • Comments and specific RIs for the gender-diverse population can be applied. • Some EHR/LIS have an option to utilize binary logic for any SOGI field difference (e.g., gender identity differing from legal sex or SAAB). |
SOGI functionality may be unavailable: • Lack of EHR/LIS capability • Limited ITb resources • Government laws/directives • Complicated informatics build • Use of gender-affirming hormones or a history of gonadectomy may not be captured by this logic. |
| Single narrow RI (overlap of existing female and male sex-specific RIs for an analyte) | • May be a useful approach for some laboratory tests if sex is unknown (e.g., legal sex in the EHR is something like unknown, *, or X) • Avoids the safety issue of having no abnormal flagging at all for analytes such as liver function assays • Interpretive comments can be appended to explain the applied RI (e.g., legal sex unknown). |
• RI is artificially constructed and may lack clinical utility. • Will result in more abnormal flagging for values that would otherwise be normal, possibly leading to flag fatigue and clinical error |
| Single wide RI (total range spanned by both male and female sex-specific ranges) | • May be a useful approach for some laboratory tests if sex is unknown (e.g., legal sex in the EHR is something like unknown, *, or X) • Best applicable to analytes such as hemoglobin with wide variability, to balance the risk of overflagging with a narrower RI while still flagging markedly abnormal results • Interpretive comments can be applied to explain the situation (e.g., legal sex unknown). |
• RI is artificially constructed and may lack clinical utility. • Risk of missing subtle abnormalities |
| No quantitative RI applied | • Useful for hormones or other analytes with high variability that make applying a single RI challenging (e.g., variation of estradiol across the menstrual cycle and during pregnancy) • Interpretive comments (including those related to gender diversity) can be applied. |
• No numeric abnormal flagging poses a risk if critical results are missed. • SOGI logic functionality required for comments related to the gender-diverse population |
| Display both female and male RIs on separate lines with sex-specific flagging | •An approach for analytes where the RI that applies to the gender-diverse population can fluctuate between the sex binary (e.g., eGFR), and can pose a high clinical risk if misinterpreted (e.g., medication dosing) | • Complicated informatics build • Abnormal flagging will be correct for at least one of the chosen sex-specified lines. • Result trending allows monitoring of gender-affirming therapy changes over time. |
| Display both female and male RIs on the same line with analyte-specific flagging | • An approach for analytes with moderate clinical risk • Both RIs are displayed, but flagging is customized per analyte relevance. • Interpretive comment can be applied. |
•Complicated informatics build • Abnormal flagging will not always be correct, but will be conservative and relevant to the analyte. |
| Display both female and male RIs on the same line with no abnormal flagging | • An approach for analytes with moderate clinical risk where flagging is not required • Interpretive comment can be applied. |
• Complicated informatics build • Flagging will not display. |
a Reference interval.
b Information technology.
Author Contributions: The corresponding author takes full responsibility that all authors on this publication have met the following required criteria of eligibility for authorship: (a) significant contributions to the conception and design, acquisition of data, or analysis and interpretation of data; (b) drafting or revising the article for intellectual content; (c) final approval of the published article; and (d) agreement to be accountable for all aspects of the article thus ensuring that questions related to the accuracy or integrity of any part of the article are appropriately investigated and resolved. Nobody who qualifies for authorship has been omitted from the list.
Authors’ Disclosures or Potential Conflicts of Interest: Upon manuscript submission, all authors completed the author disclosure form.
Research Funding: D.N. Greene received funding from Abbott Diagnostics to study hormone concentrations in people taking exogenous estradiol and Roche Diagnostics to study STI sample collection across genders.
1. Stryker S. Transgender history. New York (NY): Seal Press; 2017.
2. Walker PA, Berger JC, Green R, Laub DR, Reynolds CL, Wollman L. Standards of care: the hormonal and surgical sex reassignment of gender dysphoric persons. Palo Alto (CA): Harry Benjamin International Gender Dysphoria Association, Inc.; 1979.
3. Coleman E, Radix AE, Bouman WP, Brown GR, de Vries ALC, Deutsch MB, et al. Standards of care for the health of transgender and gender diverse people, version 8. Int J Transgend Health 2022;23:S1–259.
4. Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, Gooren LJ, Meyer WJ 3rd, Spack NP, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2009;94:3132–54.
5. Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2017;102:3869–903.
6. Rafferty J; American Academy of Pediatrics Committee on Psychosocial Aspects of Child and Family Health, Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness. Ensuring comprehensive care and support for transgender and gender-diverse children and adolescents. Pediatrics 2018;142:e20182162.
7. American Society of Plastic Surgeons. Gender surgeries: transgender facial, top and bottom procedures. https://www.plasticsurgery.org/reconstructive-procedures/gender-surgeries (Accessed April 2026).
8. American Urological Association. Transgender and gender diverse patient urologic care. https://www.auanet.org/meetings-and-education/for-medical-students/medical-students-curriculum/transgender-and-gender-diverse-patient-care (Accessed April 2026).
9. The Royal College of Pathologists of Australasia. Pathology testing for transgender and intersex individuals–best practice for medical pathology laboratories. https://www.rcpa.edu.au/Library/College-Policies/Position-Statements/Pathology-Testing-for-Transgender-and-Intersex-Ind.aspx (Accessed April 2026).
10. Lott R, Tunnicliffe J, Sheppard E, Santiago J, Hladik C, Nasim M, et al. Practical guide to specimen handling in surgical pathology. https://documents.cap.org/documents/practical-guide-specimen-handling.pdf (Accessed April 2026).
11. Leung ML, Amarillo I, Jordan D, Lebo MS, Naeem RC, Suster DI, et al. Path to health equity and improved outcomes through inclusive sex and gender data collection in genomic testing. J Mol Diagn 2025;27:677–84.
12. Theisen JG, Amarillo IE. Creating affirmative and inclusive practices when providing genetic and genomic diagnostic and research services to gender-expansive and transgender patients. J Appl Lab Med 2021;6:142–54.
13. Aaron KJ, Griner S, Footman A, Boutwell A, Van Der Pol B. Vaginal swab vs urine for detection of Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis: a meta-analysis. Ann Fam Med 2023;21:172–9.
14. Andrews AR, Kakadekar A, Greene DN, Khalifa MA, Santiago V, Schmidt RL. Histologic findings in surgical pathology specimens from individuals taking masculinizing hormone therapy for the purpose of gender transition. Arch Pathol Lab Med 2022;146:766–79.
15. Andrews AR, Kakadekar A, Schmidt RL, Murugan P, Greene DN. Histologic findings in surgical pathology specimens from individuals taking feminizing hormone therapy for the purpose of gender transition. Arch Pathol Lab Med 2022;146:252–61.
16. Angus LM, Nolan BJ, Zajac JD, Cheung AS. A systematic review of antiandrogens and feminization in transgender women. Clin Endocrinol (Oxf) 2021;94:743–52.
17. Greene DN, Schmidt RL, Winston McPherson G, Rongitsch J, Imborek KL, Dickerson JA, et al. Reproductive endocrinology reference intervals for transgender women on stable hormone therapy. J Appl Lab Med 2021;6:15–26.
18. Greene DN, Schmidt RL, Winston-McPherson G, Rongitsch J, Imborek KL, Dickerson JA, et al. Reproductive endocrinology reference intervals for transgender men on stable hormone therapy. J Appl Lab Med 2021;6:41–50.
19. Krupka E, Curtis S, Ferguson T, Whitlock R, Askin N, Millar AC, et al. The effect of gender-affirming hormone therapy on measures of kidney function: a systematic review and meta-analysis. Clin J Am Soc Nephrol 2022;17:1305–15.
20. Winston-McPherson GN, Thomas TA, Krasowski MD, Ahmed SB, Cirrincione LR, Katzman BM, et al. Estradiol concentrations for adequate gender-affirming feminizing therapy: a systematic review. LGBT Health 2025;12:477–89.
21. Antun A, Zhang Q, Bhasin S, Bradlyn A, Flanders WD, Getahun D, et al. Longitudinal changes in hematologic parameters among transgender people receiving hormone therapy. J Endocr Soc 2020;4:bvaa119.
22. Greene DN, McPherson GW, Rongitsch J, Imborek KL, Schmidt RL, Humble RM, et al. Hematology reference intervals for transgender adults on stable hormone therapy. Clin Chim Acta 2019;492:84–90.
23. Cheung AS, Bretherton I, Leemaqz SY, Perera Wedithanthrige S, Singh L, Chiang C. High-sensitivity cardiac troponin I following gender-affirming hormone therapy in transgender adults. JAMA Netw Open 2025;8:e2537205.
24. Greene DN, Schmidt RL, Christenson RH, Rongitsch J, Imborek KL, Rebuck H, et al. Distribution of high-sensitivity cardiac troponin and N-terminal pro-brain natriuretic peptide in healthy transgender people. JAMA Cardiol 2022;7:1170–4.
25. van Eeghen SA, Wiepjes CM, T'Sjoen G, Nokoff NJ, den Heijer M, Bjornstad P, van Raalte DH. Cystatin C-based eGFR changes during gender-affirming hormone therapy in transgender individuals. Clin J Am Soc Nephrol 2023;18:1545–54.
26. Turino Miranda K, Greene DN, Collister D, Krasowski MD, Ahmed SB, Cirrincione LR, et al. A holistic framework for the evaluation of kidney function in a gender-diverse landscape. Am J Kidney Dis 2024;84:232–40.
27. Turino Miranda K, Dumanski SM, Saad N, Inker LA, White CA, Delanaye P, et al. Glomerular filtration rate estimation in transgender and gender-diverse adults using gender-affirming hormone therapy: an exploratory cross-sectional study. Kidney Int 2024;106:753–6.
28. Deutsch MB, Bhakri V, Kubicek K. Effects of cross-sex hormone treatment on transgender women and men. Obstet Gynecol 2015;125:605–10.
29. Stangl TA, Wiepjes CM, Heijboer AC, den Heijer M. The influence of gender-affirming hormone therapy on serum concentrations of hormone-binding proteins. Eur J Endocrinol 2025;192:614–20.
30. Greene DN, Goldstein Z, Krasowski MD. Uncertainty in hormone monitoring of transgender and non-binary people. J Appl Lab Med 2024;9:426–9.
31. Taub RL, Ellis SA, Neal-Perry G, Magaret AS, Prager SW, Micks EA. The effect of testosterone on ovulatory function in transmasculine individuals. Am J Obstet Gynecol 2020;223:229 e1–8.
32. Chang JJ, Tran NK, Flentje A, Lubensky ME, Obedin-Maliver J, Lunn MR, Ariel D. Progestogen experience among transgender women and gender diverse adults assigned male at birth in the United States. Endocr Pract 2025;31:1449–61.
33. Humble RM, Greene DN, Schmidt RL, Winston McPherson G, Rongitsch J, Imborek KL, et al. Reference intervals for clinical chemistry analytes for transgender men and women on stable hormone therapy. J Appl Lab Med 2022;7:1131–44.
34. Defreyne J, Van de Bruaene LDL, Rietzschel E, Van Schuylenbergh J, T'Sjoen GGR. Effects of gender-affirming hormones on lipid, metabolic, and cardiac surrogate blood markers in transgender persons. Clin Chem 2019;65:119–34.
35. Rytz CL, Miranda KT, Ronksley PE, Saad N, Raj SR, Somayaji R, et al. Association between serum estradiol and cardiovascular health among transgender adults using gender-affirming estrogen therapy. Am J Physiol Heart Circ Physiol 2024;327:H340–H8.
36. SoRelle JA, Jiao R, Gao E, Veazey J, Frame I, Quinn AM, et al. Impact of hormone therapy on laboratory values in transgender patients. Clin Chem 2019;65:170–9.
37. Stangl TA, Wiepjes CM, Defreyne J, Conemans E, Fisher AD, Schreiner T, et al. Is there a need for liver enzyme monitoring in people using gender-affirming hormone therapy? Eur J Endocrinol 2021;184:513–20.
38. Wierckx K, Van Caenegem E, Schreiner T, Haraldsen I, Fisher AD, Toye K, et al. Cross-sex hormone therapy in trans persons is safe and effective at short-time follow-up: results from the European network for the investigation of gender incongruence. J Sex Med 2014;11:1999–2011.
39. Allen AN, Jiao R, Day P, Pagels P, Gimpel N, SoRelle JA. Dynamic impact of hormone therapy on laboratory values in transgender patients over time. J Appl Lab Med 2021;6:27–40.
40. Nolan BJ, Accatino MI, Angus LM, Cheung AS. Approach to prolactin monitoring and hyperprolactinaemia in transgender and gender-diverse individuals undergoing gender affirming hormone therapy. Front Endocrinol (Lausanne) 2025;16:1608108.
41. Nik-Ahd F, De Hoedt AM, Butler C, Anger JT, Carroll PR, Cooperberg MR, Freedland SJ. Prostate-specific antigen values in transgender women receiving estrogen. JAMA 2024;332:335–7.
42. Marlar RA, Gausman JN, Tsuda H, Rollins-Raval MA, Brinkman HJM. Recommendations for clinical laboratory testing for protein S deficiency: communication from the SSC committee plasma coagulation inhibitors of the ISTH. J Thromb Haemost 2021;19:68–74.
43. Reagh JJ, Zheng H, Stolz U, Parry BA, Chang AM, House SL, et al. Sex-related differences in D-dimer levels for venous thromboembolism screening. Acad Emerg Med 2021;28:873–81.
44. Franchini M, Focosi D, Pezzo MP, Mannucci PM. How we manage a high D-dimer. Haematologica 2024;109:1035–45.
45. Bachman E, Travison TG, Basaria S, Davda MN, Guo W, Li M, et al. Testosterone induces erythrocytosis via increased erythropoietin and suppressed hepcidin: evidence for a new erythropoietin/hemoglobin set point. J Gerontol A Biol Sci Med Sci 2014;69:725–35.
46. Humble RM, Imborek KL, Nisly N, Greene DN, Krasowski MD. Common hormone therapies used to care for transgender patients influence laboratory results. J Appl Lab Med 2019;3:799–814.
47. Wu AHB, Christenson RH, Greene DN, Jaffe AS, Kavsak PA, Ordonez-Llanos J, Apple FS. Clinical laboratory practice recommendations for the use of cardiac troponin in acute coronary syndrome: expert opinion from the academy of the American Association for Clinical Chemistry and the task force on clinical applications of cardiac bio-markers of the international federation of clinical chemistry and laboratory medicine. Clin Chem 2018;64:645–55.
48. Lee KK, Doudesis D, Ferry AV, Chapman AR, Kimenai DM, Fujisawa T, et al. Implementation of a high sensitivity cardiac troponin I assay and risk of myocardial infarction or death at five years: observational analysis of a stepped wedge, cluster randomised controlled trial. BMJ 2023;383:e075009.
49. Kavsak PA, Jaffe AS, Hickman PE, Mills NL, Humphries KH, McRae A, et al. Canadian institutes of health research dissemination grant on high-sensitivity cardiac troponin. Clin Biochem 2014;47:155–7.
50. Zhao Y, Izadnegahdar M, Lee MK, Kavsak PA, Singer J, Scheuermeyer F, et al. High-sensitivity cardiac troponin-optimizing the diagnosis of acute myocardial infarction/injury in women (code-mi): rationale and design for a multicenter, stepped-wedge, cluster-randomized trial. Am Heart J 2020;229:18–28.
51. Wang J, Taur A, Chen A, Wu Y-L, Lee M-S. Sex-specific cardiac troponin thresholds in transgender patients with suspected acute coronary syndrome. JAMA Netw Open 2023;6:e2337345.
52. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth universal definition of myocardial infarction. Circulation 2018;138:e618–51.
53. Regitz-Zagrosek V. Sex and gender differences in heart failure. Int J Heart Fail 2020;2:157–81.
54. Kavsak PA, Lam CSP, Saenger AK, Jaffe AS, Collinson P, Pulkki K, et al. Educational recommendations on selected analytical and clinical aspects of natriuretic peptides with a focus on heart failure: a report from the IFCC committee on clinical applications of cardiac bio-markers. Clin Chem 2019;65:1221–7.
55. Tsutsui H, Albert NM, Coats AJS, Anker SD, Bayes-Genis A, Butler J, et al. Natriuretic peptides: role in the diagnosis and management of heart failure: a scientific statement from the heart failure association of the heart failure association of the European Society of Cardiology, heart failure society of America and Japanese heart failure society. J Card Fail 2023;29:787–804.
56. van Eeghen SA, Nokoff NJ, Vosters TG, Oosterom-Eijmael MJP, Cherney DZI, van Valkengoed IGM, et al. Unraveling sex differences in kidney health and CKD: a review of the effect of sex hormones. Clin J Am Soc Nephrol 2024;20:301–10.
57. Kang SC, Jhee JH, Joo YS, Lee SM, Nam KH, Yun H-R, et al. Association of reproductive lifespan duration and chronic kidney disease in postmenopausal women. Mayo Clin Proc 2020;95:2621–32.
58. Noh JH, Koo H. Older menarche age and short reproductive period linked to chronic kidney disease risk. Medicine (Baltimore) 2019;98:e15511.
59. Kattah AG, Smith CY, Gazzuola Rocca L, Grossardt BR, Garovic VD, Rocca WA. CKD in patients with bilateral oophorectomy. Clin J Am Soc Nephrol 2018;13:1649–58.
60. van der Burgh AC, Khan SR, Neggers S, Hoorn EJ, Chaker L. The role of serum testosterone and dehydroepiandrosterone sulfate in kidney function and clinical outcomes in chronic kidney disease: a systematic review and meta-analysis. Endocr Connect 2022;11:e220061.
61. Maheshwari A, Dines V, Saul D, Nippoldt T, Kattah A, Davidge-Pitts C. The effect of gender-affirming hormone therapy on serum creatinine in transgender individuals. Endocr Pract 2022;28:52–7.
62. van Eeghen SA, Pyle L, Narongkiatikhun P, Choi YJ, Obeid W, Parikh CR, et al. Unveiling mechanisms underlying kidney function changes during sex hormone therapy. J Clin Invest 2025;135:e190850.
63. Delgado C, Baweja M, Crews DC, Eneanya ND, Gadegbeku CA, Inker LA, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN task force on reassessing the inclusion of race in diagnosing kidney disease. J Am Soc Nephrol 2021;32:2994–3015.
64. Inker LA, Eneanya ND, Coresh J, Tighiouart H, Wang D, Sang Y, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med 2021;385:1737–49.
65. Pierre CC, Marzinke MA, Ahmed SB, Collister D, Colon-Franco JM, Hoenig MP, et al. AACC/NKF guidance document on improving equity in chronic kidney disease care. J Appl Lab Med 2023;8:789–816.
66. Kidney Disease: Improving Global Outcomes CKDWG. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int 2024;105:S117–314.
67. Delanaye P, Flamant M, Vidal-Petiot E, Bjork J, Nyman U, Grubb A, et al. Discordant results between creatinine- and cystatin C-based equations for estimating GFR. Kidney Int Rep 2025;10:1248–59.
68. Pottel H, Bjork J, Rule AD, Ebert N, Eriksen BO, Dubourg L, et al. Cystatin C-based equation to estimate GFR without the inclusion of race and sex. N Engl J Med 2023;388:333–43.
69. Grams ME, Brunskill NJ, Ballew SH, Sang Y, Coresh J, Matsushita K, et al. The kidney failure risk equation: evaluation of novel input variables including eGFR estimated using the CKD-EPI 2021 equation in 59 cohorts. J Am Soc Nephrol 2023;34:482–94.
70. Liu P, Sawhney S, Heide-Jorgensen U, Quinn RR, Jensen SK, McLean A, et al. Predicting the risks of kidney failure and death in adults with moderate to severe chronic kidney disease: multinational, longitudinal, population based, cohort study. BMJ 2024;385:e078063.
71. Kauffman AS. Androgen inhibition of reproductive neuroendocrine function in females and transgender males. Endocrinology 2024;165:bqae11.
72. Xie Q, Kang Y, Zhang C, Xie Y, Wang C, Liu J, et al. The role of kisspeptin in the control of the hypothalamic-pituitary-gonadal axis and reproduction. Front Endocrinol (Lausanne) 2022;13:925206.
73. Maheshwari A, Nippoldt T, Davidge-Pitts C. An approach to nonsuppressed testosterone in transgender women receiving gender-affirming feminizing hormonal therapy. J Endocr Soc 2021;5:bvab068.
74. Greene DN, Ahmed SB, Daccarett S, Kling JM, Lorey TS, Rytz CL, et al. A comprehensive review of estradiol, progesterone, luteinizing hormone, and follicle-stimulating hormone in the context of laboratory medicine to support women's health. Clin Chem 2025;71:842–57.
75. Arrington-Sanders R, Connell NT, Coon D, Dowshen N, Goldman AL, Goldstein Z, et al. Assessing and addressing the risk of venous thromboembolism across the spectrum of gender affirming care: a review. Endocr Pract 2023;29:272–8.
76. Goldstein Z, Krasowski MD, Greene DN. Gender-affirming feminizing hormone therapy. JAMA Intern Med 2025;85:1027–8.
77. Van Caenegem E, T'Sjoen G. Bone in trans persons. Curr Opin Endocrinol Diabetes Obes 2015;22:459–66.
78. Chan KJ, Jolly D, Liang JJ, Weinand JD, Safer JD. Estrogen levels do not rise with testosterone treatment for transgender men. Endocr Pract 2018;24:329–33.
79. Ghazal K, Brabant S, Prie D, Piketty ML. Hormone immunoassay interference: a 2021 update. Ann Lab Med 2022;42:3–23.
80. Kirk D, Misita C. Spuriously elevated testosterone measurements caused by application of testosterone gel at or near the phlebotomy site. Ann Pharmacother 2013;47:e5.
81. Maggacis RA, Cheung AS, Nolan BJ. Serum estradiol concentrations with estradiol 0.06% gel in transgender and gender-diverse adults. [Epub] Clin Endocrinol (Oxf) February 14 2025, as doi: 10.1111/cen.15217
82. Nizar H, Balasanthiran A, Morganstein D, Norman B, Shotliff K. Transdermal testosterone gel. Don't take blood from the arm where gel is applied. BMJ 2010;341:c4014.
83. Pichilingue AP, Greene DN, Krasowski MD. Falsely elevated serum testosterone measurements resulting from testosterone topical gel contamination of the venipuncture site: case series and retrospective review. Heliyon 2023;9:e22819.
84. Vihtamaki T, Luukkaala T, Tuimala R. Skin contamination by oestradiol gel–a remarkable source of error in plasma oestradiol measurements during percutaneous hormone replacement therapy. Maturitas 2004;48:347–53.
85. Krasowski MD, Drees D, Morris CS, Maakestad J, Blau JL, Ekins S. Cross-reactivity of steroid hormone immunoassays: clinical significance and two-dimensional molecular similarity prediction. BMC Clin Pathol 2014;14:33.
86. Cirrincione LR, Winston McPherson G, Rongitsch J, Sadilkova K, Drees JC, Krasowski MD, et al. Sublingual estradiol is associated with higher estrone concentrations than transdermal or injectable preparations in transgender women and gender nonbinary adults. LGBT Health 2021;8:125–32.
87. Lobo RA, Cassidenti DL. Pharmacokinetics of oral 17 beta-estradiol. J Reprod Med 1992;37:77–84.
88. D'Aurizio F, Cantu M. Clinical endocrinology and hormones quantitation: the increasing role of mass spectrometry. Minerva Endocrinol 2018;43:261–84.
89. Thomas SN, French D, Jannetto PJ, Rappold BA, Clarke WA. Liquid chromatography-tandem mass spectrometry for clinical diagnostics. Nat Rev Methods Primers 2022;2:96.
90. Li D, Ferguson A, Cervinski MA, Lynch KL, Kyle PB. AACC guidance document on biotin interference in laboratory tests. J Appl Lab Med 2020;5:575–87.
91. Stieglitz HM, Korpi-Steiner N, Katzman B, Mersereau JE, Styner M. Suspected testosterone-producing tumor in a patient taking biotin supplements. J Endocr Soc 2018;2:563–9.
92. Chiu K-C, Jhan J-R, Yan H-N, Liao Y-C, Lu W-H, Lee K-Y, et al. Biotin interference in routine clinical immunoassays. Pract Lab Med 2025;45:e00472.
93. Katzman BM, Hain EA, Donato LJ, Baumann NA. Validation of a commercial reagent for the depletion of biotin from serum/plasma: a rapid and simple tool to detect biotin interference with immunoassay testing. J Appl Lab Med 2021;6:992–7.
94. Narinx N, David K, Walravens J, Vermeersch P, Claessens F, Fiers T, et al. Role of sex hormone-binding globulin in the free hormone hypothesis and the relevance of free testosterone in androgen physiology. Cell Mol Life Sci 2022;79:543.
95. Nyamaah JA, Narinx N, Antonio L, Vanderschueren D. Use of calculated free testosterone in men: advantages and limitations. Curr Opin Endocrinol Diabetes Obes 2024;31:230–5.
96. Walravens J, Adaway J, Reyns T, Narinx N, Nyamaah JA, Antonio L, et al. Variability in SHBG assays and the effect thereof on calculated estimates of free testosterone. Ann Clin Biochem 2025;62:493–500.
97. Naranjo AR, Krasowski MD, Hamdan A, O'Connor K, Carter C, Chen J, Greene DN. Reflex strategy to ensure accurate total testosterone results from consumer initiated, self-collected capillary samples. Clin Chim Acta 2024;558:119676.
98. Castellano E, Crespi C, Dell'Aquila C, Rosato R, Catalano C, Mineccia V, et al. Quality of life and hormones after sex reassignment surgery. J Endocrinol Invest 2015;38:1373–81.
99. Sofer Y, Yaish I, Yaron M, Bach MY, Stern N, Greenman Y. Differential endocrine and metabolic effects of testosterone suppressive agents in transgender women. Endocr Pract 2020;26:883–90.
100. Shieh A, Greendale GA, Cauley JA, Karvonen-Gutierrez C, Crandall CJ, Karlamangla AS. Estradiol and follicle-stimulating hormone as predictors of onset of menopause transition-related bone loss in pre- and perimenopausal women. J Bone Miner Res 2019;34:2246–53.
101. Prior JC. Progesterone is important for transgender women's therapy-applying evidence for the benefits of progesterone in ciswomen. J Clin Endocrinol Metab 2019;104:1181–6.
102. Wierckx K, Gooren L, T'Sjoen G. Clinical review: breast development in trans women receiving cross-sex hormones. J Sex Med 2014;11:1240–7.
103. Caanen MR, Soleman RS, Kuijper EA, Kreukels BP, De Roo C, Tilleman K, et al. Antimullerian hormone levels decrease in female-to-male transsexuals using testosterone as cross-sex therapy. Fertil Steril 2015;103:1340–5.
104. Reisman T, Safer JD. Are adrenal androgens altered by gender-affirming hormone therapy? J Clin Endocrinol Metab 2023;108:e191–2.
105. Yaish I, Tordjman K, Amir H, Malinger G, Salemnick Y, Shefer G, et al. Functional ovarian reserve in transgender men receiving testosterone therapy: evidence for preserved anti-Mullerian hormone and antral follicle count under prolonged treatment. Hum Reprod 2021;36:2753–60.
106. Cao J, Donato L, El-Khoury JM, Goldberg A, Meeusen JW, Remaley AT. ADLM guidance document on the measurement and reporting of lipids and lipoproteins. J Appl Lab Med 2024;9:1040–56.
107. Poteat TC, Rich AJ, Jiang H, Wirtz AL, Radix A, Reisner SL, et al. Cardiovascular disease risk estimation for transgender and gender-diverse patients: cross-sectional analysis of baseline data from the lite plus cohort study. AJPM Focus 2023;2:100096.
108. Vecchiato M, Neunhaeuserer D, Palermi S, Biffi A, Scala A, Ermolao A. The challenge of accurate cardiovascular risk assessment in gender-affirming individuals. Eur J Prev Cardiol 2025;33:453–5.
109. Hashemi L, Zhang Q, Getahun D, Jasuja GK, McCracken C, Pisegna J, et al. Longitudinal changes in liver enzyme levels among transgender people receiving gender affirming hormone therapy. J Sex Med 2021;18:1662–75.
110. Tienforti D, Savignano G, Spagnolo L, Di Giulio F, Baroni MG, Barbonetti A. Biochemical liver damage during gender affirming therapy in trans adults assigned female at birth: a meta-analysis. J Endocrinol Invest 2025;48:161–71.
111. Melmed S, Casanueva FF, Hoffman AR, Kleinberg DL, Montori VM, Schlechte JA, et al. Diagnosis and treatment of hyperprolactinemia: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2011;96:273–88.
112. Bisson JR, Chan KJ, Safer JD. Prolactin levels do not rise among transgender women treated with estradiol and spironolactone. Endocr Pract 2018;24:646–51.
113. Burinkul S, Panyakhamlerd K, Suwan A, Tuntiviriyapun P, Wainipitapong S. Anti-androgenic effects comparison between cyproterone acetate and spironolactone in transgender women: a randomized controlled trial. J Sex Med 2021;18:1299–307.
114. Gava G, Cerpolini S, Martelli V, Battista G, Seracchioli R, Meriggiola MC. Cyproterone acetate vs leuprolide acetate in combination with transdermal oestradiol in transwomen: a comparison of safety and effectiveness. Clin Endocrinol (Oxf) 2016;85:239–46.
115. Gava G, Mancini I, Alvisi S, Seracchioli R, Meriggiola MC. A comparison of 5-year administration of cyproterone acetate or leuprolide acetate in combination with estradiol in transwomen. Eur J Endocrinol 2020;183:561–9.
116. Raven LM, Guttman-Jones M, Muir CA. Hyperprolactinemia and association with prolactinoma in transwomen receiving gender affirming hormone treatment. Endocrine 2021;72:524–8.
117. Fleming J, Grasso C, Mayer KH, Reisner SL, Potter J, Streed CG Jr. Gender-affirming hormone therapy and cervical cancer screening rates in transgender men and nonbinary people: a cross-sectional study from a Boston Community Health Center. LGBT Health 2024;11:514–21.
118. Fosmore CL, Sullivan S, Brouwer AF, Goold SD, Reisner SL, Fendrick AM, Harper DM. Strategies to optimize cervical cancer screening rates among transgender and gender-diverse people assigned female at birth. J Gen Intern Med 2024;39:3333–8.
119. Wang JC, Peitzmeier S, Reisner SL, Deutsch MB, Potter J, Pardee D, Hughto JMW. Factors associated with unsatisfactory pap tests among sexually active trans masculine adults. LGBT Health 2023;10:278–86.
120. Moatamed NA, Barco AD, Yang SE, Ying Y, Zhang S, Rodriguez EF. Clinical history of female-to-male transgender patients is needed to avoid misinterpretation of cervical papanicolaou tests. Cytopathology 2023;34:120–9.
121. Torous VF. Cervicovaginal papanicolaou tests in transgender men: cytomorphologic alterations, interpretation considerations, and clinical implications. Cancer Cytopathol 2023;131:626–36.
122. Williams MPA, Kukkar V, Stemmer MN, Khurana KK. Cytomorphologic findings of cervical pap smears from female-to-male transgender patients on testosterone therapy. Cancer Cytopathol 2020;128:491–8.
123. El-Zein M, Franco EL. Evolution and future of cervical cancer screening: from cytology to primary HPV testing and the impact of vaccination. Expert Rev Mol Diagn 2025;25:157–64.
124. Koliopoulos G, Nyaga VN, Santesso N, Bryant A, Martin-Hirsch PP, Mustafa RA, et al. Cytology versus HPV testing for cervical cancer screening in the general population. Cochrane Database Syst Rev 2017;8:CD008587.
125. Costa S, Verberckmoes B, Castle PE, Arbyn M. Offering HPV self-sampling kits: an updated meta-analysis of the effectiveness of strategies to increase participation in cervical cancer screening. Br J Cancer 2023;128:805–13.
126. McDowell M, Pardee DJ, Peitzmeier S, Reisner SL, Agenor M, Alizaga N, et al. Cervical cancer screening preferences among trans-masculine individuals: patient-collected human papillomavirus vaginal swabs versus provider-administered pap tests. LGBT Health 2017;4:252–9.
127. Petrik AF, Rivelli JS, Firemark AJ, Johnson CA, Locher BW, Gille S, et al. A qualitative assessment of the acceptability of human papillomavirus self-sampling and informational materials among diverse populations. Cancer Med 2024;13:e70033.
128. Howard MF, Fyffe-Freil RC, Pierre CC, Maku HO, Di Costanzo S, Lorey TS, Greene DN. Self-collection for primary HPV screening using dry swabs: a review of clinical performance, laboratory considerations, and patient preferences. J Clin Microbiol 2026;64:e0076724.
129. Khan A, Culbreath K, Goldstein Z, Greene DN. Access barriers in testing for sexually transmitted infections across gender and sexual identities. Clin Lab Med 2024;44:647–63.
130. Nik-Ahd F, De Hoedt A, Butler C, Anger JT, Carroll PR, Cooperberg MR, Freedland SJ. Prostate cancer in transgender women in the Veterans Affairs Health System, 2000–2022. JAMA 2023;329:1877–9.
131. Nik-Ahd F, Anger JT, Cooperberg MR, Freedland SJ. Prostate cancer is not just a man's concern—the use of PSA screening in transgender women. Nat Rev Urol 2023;20:323–4.
132. Iwamoto SJ, Grimstad F, Irwig MS, Rothman MS. Routine screening for transgender and gender diverse adults taking gender-affirming hormone therapy: a narrative review. J Gen Intern Med 2021;36:1380–9.
133. Baraban E, Ding CC, White M, Vohra P, Simko J, Boyle K, et al. Prostate cancer in male-to-female transgender individuals: histopathologic findings and association with gender-affirming hormonal therapy. Am J Surg Pathol 2022;46:1650–8.
134. Hiransuthikul A, Janamnuaysook R, Sungsing T, Jantarapakde J, Trachunthong D, Mills S, et al. High burden of chlamydia and gonorrhoea in pharyngeal, rectal and urethral sites among Thai transgender women: implications for anatomical site selection for the screening of STI. Sex Transm Infect 2019;95:534–9.
135. McCartney DJ, Pinheiro TF, Gomez JL, Carvalho PGC, Veras MA, Mayaud P. Acceptability of self-sampling for etiological diagnosis of mucosal sexually transmitted infections (STIs) among transgender women in a longitudinal cohort study in Sao Paulo, Brazil. Braz J Infect Dis 2022;26:102356.
136. Pitasi MA, Kerani RP, Kohn R, Murphy RD, Pathela P, Schumacher CM, et al. Chlamydia, gonorrhea, and human immunodeficiency virus infection among transgender women and transgender men attending clinics that provide sexually transmitted disease services in six US cities: results from the sexually transmitted disease surveillance network. Sex Transm Dis 2019;46:112–7.
137. Tordoff DM, Dombrowski JC, Ramchandani MS, Barbee LA. Trans-inclusive sexual health questionnaire to improve human immunodeficiency virus/sexually transmitted infection (STI) care for transgender patients: anatomic site-specific STI prevalence and screening. Clin Infect Dis 2023;76:e736–43.
138. United States Food & Drug Administration Center for Biologics Evaluation and Research. Implementation of acceptable full-length and abbreviated donor history questionnaires and accompanying materials for use in screening donors of blood and blood components: Guidance for industry. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/implementation-acceptable-full-length-and-abbreviated-donor-history-questionnaires-and-accompanying (Accessed April 2026).
139. Domingue MP, Camirand Lemyre F, Aube E, Renaud C, Thibeault C, Caruso J, et al. Risk of transfusion-related acute lung injury and human immunodeficiency virus associated with donations from trans donors in Quebec, Canada. Vox Sang 2022;117:1070–7.
140. Reynolds V, Van Buren NL, Gorlin JB. Confronting the challenge of gender nonconforming donors: a blood center's three-year experience. Transfusion 2023;63:1284–9.
141. Haw J, Butler-Foster T, Murray B, Lapierre D, Bosse J, Edwards J, et al. Advancing gender inclusivity for two-spirit, trans, nonbinary and other gender-diverse blood and plasma donors. Vox Sang 2024;119:409–16.
142. Thorpe R, Jensen K, Masser B, Bentley P, Dryden T, Forrest E, et al. Understanding community perspectives for advancing inclusion of trans and gender-diverse people in blood donation in Australia. Vox Sang 2025;120:447–54.
143. Mays JA, Greene DN, Metcalf RA, Pagano MB. Transfusion support for transgender men of childbearing age. Transfusion 2018;58:823–5.
144. Fedor J, Krywanczyk A, Redgrave A. Gender identity in forensic death investigation: a narrative review and suggested guidelines for documenting and reporting. Am J Forensic Med Pathol 2024;45:231–41.
145. Walters JK, Mew MC, Repp KK. Transgender and nonbinary deaths investigated by the state medical examiner in the Portland, Oregon, metro area and their concordance with vital records, 2011–2021. J Public Health Manag Pract 2023;29:64–70.
146. Dinno A. Homicide rates of transgender individuals in the United States: 2010–2014. Am J Public Health 2017;107:1441–7.
147. Haas AP, Lane AD, Blosnich JR, Butcher BA, Mortali MG. Collecting sexual orientation and gender identity information at death. Am J Public Health 2019;109:255–9.
148. Blosnich JR, Butcher BA, Mortali MG, Lane AD, Haas AP. Training death investigators to identify decedents’ sexual orientation and gender identity: a feasibility study. Am J Forensic Med Pathol 2022;43:40–5.
149. California Health and Safety Code. California gender recognition act. §102875. 2023. https://codes.findlaw.com/ca/health-and-safety-code/hsc-sect-102875/ (Accessed April 2026).
150. New York Administrative Code. Sex designation on death records. §17-166.1. 2025. https://codelibrary.amlegal.com/codes/newyorkcity/latest/NYCadmin/0-0-0-27606 (Accessed April 2026).
151. New Jersey Revised Statutes. Contents of death certificate. §26:6-7. 2024. https://law.justia.com/codes/new-jersey/title-26/section-26-6-7/ (Accessed April 2026).
152. Colorado Revised Statutes. Gender identity certificate of death. §25-2-110. 2025. https://law.justia.com/codes/colorado/title-25/vital-statistics/article-2/section-25-2-110/ (Accessed April 2026).
153. District of Columbia Official code. Death certificate gender identity recognition amendment act of 2016. §7-211. 2016. https://code.dccouncil.gov/us/dc/council/laws/21-258 (Accessed April 2026).
154. McCaffrey RL, James AJ, Torres-Guzman RA, Addae JK, Sullivan LE, Dash E, et al. Incidence of high risk and malignant pathological findings in transgender and gender diverse individuals undergoing gender-affirming mastectomy. Ann Surg Oncol 2024;31:8086–92.
155. Huynh V, Conroy M, Carroll EF, Cortina CS. Contemporary considerations for breast cancer risk and screening in transgender, nonbinary, and gender-diverse populations. Curr Breast Cancer Rep 2025;17:8.
156. Cornejo KM, Oliva E, Crotty R, Sadow PM, Devins K, Wintner A, Wu C-L. Clinicopathologic features and proposed grossing protocol of orchiectomy specimens performed for gender affirmation surgery. Hum Pathol 2022;127:21–7.
157. da Silva ED, Riveri RC, Spritzer PM, Fighera TM. Uterine changes in transgender men receiving testosterone therapy. Eur J Endocrinol 2024;191:175–82.
158. Khalifa MA, Toyama A, Klein ME, Santiago V. Histologic features of hysterectomy specimens from female-male transgender individuals. Int J Gynecol Pathol 2019;38:520–7.
159. Grimstad FW, Fowler KG, New EP, Ferrando CA, Pollard RR, Chapman G, et al. Uterine pathology in transmasculine persons on testosterone: a retrospective multicenter case series. Am J Obstet Gynecol 2019;220:257.e1–7.
160. Nucci MR, Ferry JA, Young RH. Ectopic prostatic tissue in the uterine cervix: a report of four cases and review of ectopic prostatic tissue. Am J Surg Pathol 2000;24:1224–30.
161. Pirtea P, Ayoubi JM, Desmedt S, T'Sjoen G. Ovarian, breast, and metabolic changes induced by androgen treatment in transgender men. Fertil Steril 2021;116:936–42.
162. Dasaraju S, Klein ME, Murugan P, Farooqui M, Khalifa MA. Microscopic features of vaginectomy specimens from transgender patients. Am J Clin Pathol 2022;158:639–45.
163. Chaum M, Grossi S, Chen J, Hu V, Ray E, Giuliano A, Bose S. Masculinizing hormone therapy effect on breast tissue: changes in estrogen and androgen receptors in transgender female-to-male mastectomies. Breast 2023;72:103596.
164. Wolters EA, Rabe KE, Siegel L, Butts J, Klein ME. Histopathologic features of breast tissue from transgender men and their associations with androgen therapy. Am J Clin Pathol 2023;159:43–52.
165. Goodwin WE, Cummings RH. Squamous metaplasia of the verumontanum with obstruction due to hypertrophy: long-term effects of estrogen on the prostate in an aging male-to-female transsexual. J Urol 1984;131:553–4.
166. Lips P, Asscheman H, Uitewaal P, Netelenbos JC, Gooren L. The effect of cross-gender hormonal treatment on bone metabolism in male-to-female transsexuals. J Bone Miner Res 1989;4:657–62.
167. Kakadekar A, Greene DN, Schmidt RL, Khalifa MA, Andrews AR. Nonhormone-related histologic findings in postsurgical pathology specimens from transgender persons. Am J Clin Pathol 2022;157:337–44.
168. Becker T, Chin M, Bates N. Measuring sex, gender identity, and sexual orientation. Washington (DC): National Academies; 2022.
169. Chittalia AZ, Marney HL, Tavares S, Warsame L, Breese AW, Fisher DL, et al. Bringing cultural competency to the EHR: lessons learned providing respectful, quality care to the LGBTQ community. AMIA Annu Symp Proc 2020;2020:303–10.
170. Imborek KL, Nisly NL, Hesseltine MJ, Grienke J, Zikmund TA, Dreyer NR, et al. Preferred names, preferred pronouns, and gender identity in the electronic medical record and laboratory information system: is pathology ready? J Pathol Inform 2017;8:42.
171. Maragh-Bass AC, Torain M, Adler R, Schneider E, Ranjit A, Kodadek LM, et al. Risks, benefits, and importance of collecting sexual orientation and gender identity data in healthcare settings: a multi-method analysis of patient and provider perspectives. LGBT Health 2017;4:141–52.
172. Grutman AJ. Use of chosen names in electronic health records to promote transgender inclusivity. J Am Med Inform Assoc 2023;30:1219–21.
173. Burgess C, Kauth MR, Klemt C, Shanawani H, Shipherd JC. Evolving sex and gender in electronic health records. Fed Pract 2019;36:271–7.
174. Cahill S, Singal R, Grasso C, King D, Mayer K, Baker K, Makadon H. Do ask, do tell: high levels of acceptability by patients of routine collection of sexual orientation and gender identity data in four diverse American community health centers. PLoS One 2014;9:e107104.
175. Callahan EJ, Sitkin N, Ton H, Eidson-Ton WS, Weckstein J, Latimore D. Introducing sexual orientation and gender identity into the electronic health record: one academic health center's experience. Acad Med 2015;90:154–60.
176. Thompson HM, Kronk CA, Feasley K, Pachwicewicz P, Karnik NS. Implementation of gender identity and assigned sex at birth data collection in electronic health records: where are we now? Int J Environ Res Public Health 2021;18:6599.
177. Gupta S, Imborek KL, Krasowski MD. Challenges in transgender healthcare: the pathology perspective. Lab Med 2016;47:180–8.
178. Kronk CA, Everhart AR, Ashley F, Thompson HM, Schall TE, Goetz TG, et al. Transgender data collection in the electronic health record: current concepts and issues. J Am Med Inform Assoc 2022;29:271–84.
179. Dubin S, Cook T, Liss A, Doty G, Moore K, Greene R, et al. Comparing electronic health record domains’ utility to identify transgender patients. Transgend Health 2022;7:78–84.
180. Hines NG, Greene DN, Imborek KL, Krasowski MD. Patterns of gender identity data within electronic health record databases can be used as a tool for identifying and estimating the prevalence of gender-expansive people. JAMIA Open 2023;6:ooad042.
181. Mayer KH, Peretti M, McBurnie MA, King D, Smith NX, Crawford P, et al. Wide variability in documentation of sexual orientation, gender identity, and preventive health screenings in a diverse sample of U.S. Community Health Centers. LGBT Health 2022;9:571–81.
182. Connolly DJ, Dewan H, Holland A. Rising transphobia and disparities in drug-related harm experienced by transgender and gender-diverse people. Harm Reduct J 2025;22:57.
183. Connolly DJ, Meads C, Wurm A, Brown C, Bayliss J, Oakes-Monger TC, Berner AM. Transphobia in the United Kingdom: a public health crisis. Int J Equity Health 2025;24:155.
184. Rafique Z, Riaz S, Habib S. The debilitating impact of transphobia on health care services: the moderated mediation model of transphobia, minority stress, social exclusion, and access to health care among people who are transgender. Int J Soc Determinants Health Health Serv 2025;55:402–14.
185. Suen LW, Lunn MR, Sevelius JM, Flentje A, Capriotti MR, Lubensky ME, et al. Do ask, tell, and show: contextual factors affecting sexual orientation and gender identity disclosure for sexual and gender minority people. LGBT Health 2022;9:73–80.
186. Walsh AR, Spiars DE, Loder C, Dove-Medows E, Kalpakjian C, Hess A, et al. Sexual and gender identity-associated disparities in university students’ experiences with inappropriate, disrespectful, and coercive health care. LGBT Health 2025;12:295–305.
187. Basil NN, Ambe S, Ekhator C, Fonkem E. Health records database and inherent security concerns: a review of the literature. Cureus 2022;14:e30168.
188. Khanijahani A, Iezadi S, Agoglia S, Barber S, Cox C, Olivo N. Factors associated with information breach in healthcare facilities: a systematic literature review. J Med Syst 2022;46:90.
189. Maku H, Pierre CC, Greene DN, Henderson E, Rogers CL, Whitley C, Winston-McPherson GN. Creation and evaluation of a gender diversity focused cultural competency training for phlebotomists: study protocol for a randomized controlled trial. Heliyon 2025;11:e42023.
190. Goldstein Z, Corneil TA, Greene DN. When gender identity doesn't equal sex recorded at birth: the role of the laboratory in providing effective healthcare to the transgender community. Clin Chem 2017;63:1342–52.
191. Jessen K, Wijeratne N, Connell A. The intersection of the laboratory and transgender care. Crit Rev Clin Lab Sci 2025;62:347–62.
192. Patel K, Lyon ME, Luu HS. Providing inclusive care for transgender patients: capturing sex and gender in the electronic medical record. J Appl Lab Med 2021;6:210–8.
193. Advocates for Trans Equality. ID documents center. https://transequality.org/documents (Accessed April 2026).
194. Movement Advancement Project. Identity document laws and policies. https://www.lgbtmap.org/equality-maps/identity_documents (Accessed April 2026).
195. Cardillo AB, Chen D, Haghi N, O'Donnell L, Jhang J, Testa PA, Genes N. Reference ranges for all: implementing reference ranges for transgender and nonbinary patients. Appl Clin Inform 2024;15:1093–6.
196. Krasowski MD, Hines NG, Imborek KL, Greene DN. Impact of sex used for assignment of reference intervals in a population of patients taking gender-affirming hormones. J Clin Transl Endocrinol 2024;36:100350.
197. Stoffel M, Luu HS, Krasowski MD. Laboratory informatics approaches to improving care for gender- diverse patients. Clin Lab Med 2024;44:575–90.
198. Freilich J, Kesselheim AS. Data manipulation within the US Federal Government. Lancet 2025;406:227–8.
199. Halem J, Manion J, Streed CG Jr. A legacy of cruelty to sexual and gender minority groups. N Engl J Med 2024;391:385–91.
Guidance Documents are brought to you by the